Business of Aging
Glenmeadow Renovates, Responds to Lifestyle Changes

Tim Cotz, president and CEO of Glenmeadow
Of course, he’s impressed with an octogenarian who is active on Facebook, but he said he’s even more pleased to see one of his staff reaching out to her, because it’s the personal bonds among the staff and residents that make Glenmeadow — an independent- and assisted-living complex in Longmeadow — feel like home.
In fact, Cotz can be found pouring coffee every weekday morning at 7 a.m., walking around opening shades for more light, and pouring glasses of chardonnay at a late Friday afternoon cocktail hour; his daily, hands-on style is a physical illustration of what he expects of his 110 employees in all their different roles. This philosophy, and an open ear to requests for change, have helped Glenmeadow grow successfully over the past 20 years, weather the Great Recession, and recently complete a $4 million renovation (more on that later).
Cotz describes Glenmeadow as “unique” in the business of senior living because it’s a stand-alone, nonprofit facility, while most of its competition is religious-based, for-profit, owned by private entities, or merged into large conglomerates.
He told BusinessWest that, while he’s always worked to enhance services and meet the expectations of his residents and their families, it’s a much more vocal demographic these days.
“I don’t think we can ever be a place where we say, ‘this is what we do, this is what we offer, that’s what it is,’” said Cotz, who noted that the organization’s original managers, which became a board in 1985, was long run by a group of ladies; in its 130-year history, Cotz is the first male to have the leadership role in Glenmeadow. “We’re ever-evolving.”
As another example, he mentioned a new addition to the staff, whose role is to help residents with their technology needs. Requests for assistance with iPads, iPhones, laptops, and the general need to keep up with social media is as important to residents, he said, as it is to everyone else today.
When Glenmeadow opened its new facility 17 years ago, “we had one person here with their own computer,” Cotz explained. “Now we have wi-fi throughout the building, and a majority of the folks have computers, so we’re looking at how we continue to enhance those services.”
For this issue’s focus on the business of aging, BusinessWest toured Glenmeadow to learn more about an elder residence with a long history in Greater Springfield, and how that nonprofit is catering to a demographic requesting amenities and programs reflecting a younger mindset than ever before.
Welcome Home
Working in long-term care since 1970, Cotz started as an orderly in college, and graduated from Hartwick College with a bachelor’s degree in healthcare before earning his master’s from George Washington University.
From 1982 to 1988, he served as executive director of the Geriatric Authority of Holyoke, then led Berkshire Health Systems in Pittsfield for five years, before transitioning to Glenmeadow, which at the time was located in downtown Springfield.

Tim Cotz said the $4 million in recent renovations includes the Doorstop Café, a popular meeting place for residents as well as visiting friends.
“Every city at the time had a ‘poor farm,’ and that’s where old people went,” Cotz told BusinessWest. “But the citizenry of Springfield felt that they deserved a better option.”
The first structure was a home behind the current Red Rose Pizza in Springfield’s South End, which then moved to a mansion on the corner of Chestnut and Carew streets (the building is now used for alcohol and drug rehabilitation services), and by the 1960s the name was changed to Chestnut Knoll.
When the facility needed more space, it purchased a 20-acre plot of land from Daniel O’Connell’s Sons in 1993, just over the Springfield line in Longmeadow, and construction for the current facility was completed in 1997. The richly landscaped campus and buildings now boast 113 independent apartments (14 more were added in 2000 to the original 89 units), boasting full kitchens and baths, plus 34 assisted-living apartments with kitchenettes.
Demand for units has been fairly consistent over the past two decades, Cotz said. The recession impacted the nonprofit a bit in 2008 and 2009, causing the waiting list to shrink, but residents have consistently filled the apartments. After the recession, not only did the waiting list fill up again, the changing style of how seniors want to live created demands of a different sort.
Great Expectations
Specifically, Cotz pointed out two societal shifts that have affected Glenmeadow over the past decade. First is the trend toward ‘aging in place,’ which the facility turned into a revenue generator in 2001 with the introduction of Glenmeadow at Home, a non-medical, private-duty, home-healthcare company for those living there.
“People are living so much longer and living healthier, and typically there are periods where they need some additional support. So now we can hire our own staff, train them, do the background, and supervise them,” he explained. Residents also have the option to hire outside workers for those extra services, if they so choose.
The goal is to provide non-medical services that help elders stay comfortably in their home, which includes companionship, handyman service, transportation, meals, dog walking, and more. By 2003, Glenmeadow at Home expanded to caring for anyone 62 and older in the Greater Springfield community. Calls to clients’ personal physicians for medical attention are part of the services, and that eventually evolved into care management in the home to coordinate all the services that an elder would need as their medical care requirements increase. Today, Glenmeadow at Home employs 80.
The second trend Cotz has observed is a renewed focus on fitness and lifestyle programming.
“The population we’re serving is clearly looking for more options for wellness, so much so that 83% of the people in this building exercise regularly,” he explained, which has led to an expansion of wellness services on site.
“When we opened 17 years ago, we had a room about this size, and if people brought an exercise bike, we’d store it in there,” Cotz said, pointing around his office, which comfortably holds a desk, a table, and two easy chairs. “Well, now we have three trainers on staff, Nautilus equipment, and numerous exercise classes each day, from stretching to balance to Tai Chi, PiYo [a blend of Pilates and yoga], and aquasize.”
This attention to physical and mental wellness, Cotz told BusinessWest, is due to behavioral differences among three generations: the Silent Generation (born 1925-1944) and the GI Generation (1905-1924), which together which make up a large portion of Glenmeadow’s older residents, and the older edge of the Baby Boom Generation (1945-1964), who are now entering the facility or on the waiting list.
“They are very different populations; the expectations of people we’re serving are changing,” said Cotz. “My parents’ generation, the GI population, were kind of ‘give me a cot and a cup of coffee, and I’m good to go.’ But the people in their early 70s coming in clearly have higher expectations in terms of amenities, programs, and services.”
The standard independent-living facility — with individual living units, one large dining room, and some separate rooms for a lounge, library, puzzles, and crafts — are from a bygone era. Now, the demand for more contemporary open space and more choices for meal times has changed the entire look and feel of Glenmeadow’s first floor.
The complex recently invested $4 million in renovations to tear down interior walls, open up meeting rooms, add more windows for natural light, expand the wellness area, and split the formal dining room to create the casual Doorstop Café, as well as more administrative space for the growing Glenmeadow at Home.
Living Social
Another concern is the alarming trend of cognitive loss, ranging from general senility to vascular-related dementia to Alzheimer’s disease. Both Glenmeadow and Glenmeadow at Home aim to identify the first signs of impairment and the supports necessary to keep people independent for as long as possible.
While Glenmeadow is a private-pay business, the nonprofit accepts donations through requests and estates, and has an investment portfolio of $15 million. Those investments can help those that outlive their resources; Cotz said the facility has never discharged anyone due to inability to pay.
In addition, a few years ago, Glenmeadow began offering the use of its facilities to non-residents for only $25 per month. With little advertising, membership escalated to more than 80 people after renovations were completed last fall. Members take advantage of the pool, use the fitness programs and equipment, and grab soup or coffee at the Doorstop Café, Cotz said. “It allows the public to realize first-hand what could be their next home.”
That’s certainly worth a Facebook ‘like’ or two.
Elizabeth Taras can be reached at [email protected]
Breakdown of Cartilage Between Joints Leads to Osteoarthritis
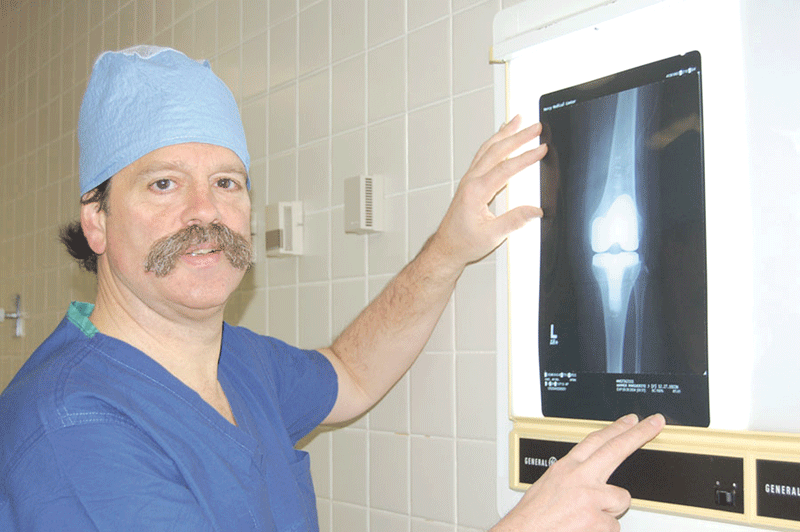
Dr. Leonard Wagner says the most noticeable symptom of osteoarthritis is joint pain, but people also experience tenderness, stiffness, and loss of flexibility or range of motion.
“There are a lot of people who never develop arthritis, and there are others who do have it whose lives can be markedly improved with appropriate attention,” said orthopedic surgeon Dr. Leonard Wagner of Springfield.
Dr. James Schumacher agrees. “Osteoarthritis a very common disorder, and if you look hard enough, you can find it in everyone 40 or older, particularly in the spine,” said the rheumatologist from Riverbend Medical Group in Chicopee. “But the progression of the disease is very slow and takes place over decades.”
OA can affect the neck, back, hip, knee, shoulder, feet, thumb, or fingers. “Arthritis means inflammation of the joint, and osteoarthritis can affect just one or two joints, compared to other types that can involve the entire body,” Wagner said. The most noticeable symptom is pain in or around the joint, but people can also experience tenderness and/or stiffness and loss of flexibility or range of motion. Some also report a grating sensation or sound in the joint when they move.
The problem is caused by a breakdown of cartilage, which is a tough, elastic, fibrous connective tissue between the bones in the joint that provides them with cushioning. When it becomes too thin, the bones rub together, which leads to inflammation, stiffness, pain, and loss of movement.
But Schumacher says pain increases gradually and is dependent on many factors, such as a person’s weight and how much stress is put on the joint. In addition, what doctors find on X-rays or magnetic-resonance imaging does not necessarily correlate to the degree of pain people experience, he told BusinessWest.
However, some factors, such as obesity, make the problem worse, especially when the knees are affected. Wagner says every extra pound translates to three to four pounds of extra stress on the knee in people with OA. “So if you gain 10 pounds, the knee thinks you gained 40 pounds.”
Keeping active is important, but can be difficult because the more pain a person has, the less likely they are to exercise. “It’s a downward spiral,” Schumacher said. “If you can’t exercise, it’s easy to gain weight, and the more you gain, the more it hurts to exercise.”
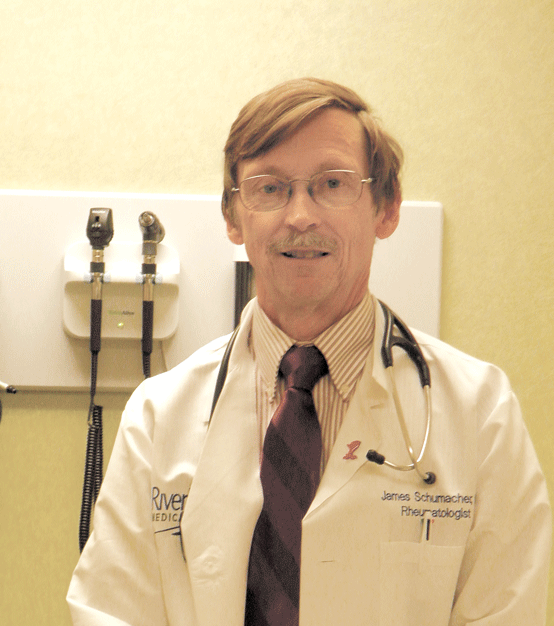
Dr. James Schumacher says the progression of osteoarthritis can be very slow, gradually worsening over decades.
Progressive Condition
In addition to obesity, which can make OA worse, other factors put people at risk for the condition. “We don’t really know why osteoarthritis develops, but it is believed that genetics may play a role,” Schumacher said.
There is also a correlation between past injuries and symptoms. They include sports mishaps, car accidents, or a bad fall. In fact, the Arthritis Foundation says researchers have determined that 10 to 20 years after a traumatic injury to the knee — such as an ACL or meniscus tear — about 50% of patients will develop OA.
“The knee is very prone to injury,” Schumacher said. “But any joint can be involved, and if there is a deformity or slight variation in normal structure, it may lead to osteoarthritis.”
The condition occurs over time, and is often referred to as ‘wear-and-tear’ arthritis. Wagner explained that cartilage has a very slippery surface. That surface, combined with a small amount of fluid, keeps the joints lubricated.
However, as the cartilage degenerates or thins out, its surface becomes more like sandpaper, which prevents the bones from gliding easily. As the thinning progresses, they can begin to rub together. “It leads to inflammation, and as the body produces more inflamed cells, there is more and more pain and stiffness,” he said.
At first, pain may be infrequent and only occur with weather changes or when engaging in a strenuous activity. “But as time goes on, the symptoms become more of an issue,” Wagner said, adding that knees tend to be particularly painful because they are weight bearing and people cannot avoid using them because they need to walk.
However, there are measures people can take to help prevent OA. They include maintaining a healthy weight, taking care of injuries when they happen, and staying active. “You don’t need to go to the gym four times a week,” he said. “People just need to keep moving. Every walk you take or every time you take the stairs will help.”
Schumacher agrees. “All exercise counts, even walking from the far end of a parking lot. People who do this are actually getting good exercise. If you only do it once in a while, it will be more difficult, but a small amount is better than nothing, because the body does remember.”
Treatment Options
Wagner says there are a number of modalities used to cope with disabling pain. Many people use canes or walkers. “They can also get injections which decrease inflammation. And certain anti-inflammatory medications can also help to decrease inflammation and discomfort and may make your life more enjoyable. A lot of people take ibuprofen or Aleve and find it is beneficial. But it is important to pay attention to the directions because there is a potential of irritating the stomach.”
Schumacher agreed, and said people who take prescription medications or have other medical conditions should check with their doctor before embarking on a self-treatment plan of over-the-counter medications, as drug interactions and stomach inflammation can occur. “The doctor needs to look at the whole picture and decide what is a reasonable risk.”
Both physicians also urge people with pain that continues over time to visit their physician. “It’s useful to talk to your doctor about your symptoms, get a diagnosis, and find out what treatment is best,” Schumacher said. “A physical exam can detect changes in function, range of motion, and tenderness. We also use X-rays and MRIs to test the severity and extent of osteoarthritis, although there is a lot of variation in symptoms compared to these studies. But our aim is do what we can through medical management.”
However, Wagner says many people fail to schedule a doctor’s visit because they assume they know what is wrong with them and what the physician will prescribe.
“But just because you have pain in a joint doesn’t mean it’s arthritis or you need a particular treatment plan,” he explained. “For example, it’s possible to have pain and swelling in a knee from torn cartilage, even though the person may not remember getting injured. Or someone may have worked too hard in the garden and have tendinitis, which rest and over-the-counter medication will take care of.”
Surgery provides relief for many people, but is not scheduled until other treatment options are exhausted. “Joint replacement is usually the last option,” Schumacher said. “It is a big procedure, and it’s expensive, but for those who are barely able to get around, it can be quite helpful.”
Future Outlook
Osteoarthritis stems from a variety of causes, but is definitely associated with aging. “It is seen in younger people, but that is usually the result of injury or previous trauma to the joint,” Schumacher noted.
And although there is a lot of interest in what makes cartilage deteriorate, it is hard to study.
“Our understanding of why and how osteoarthritis happens is not very good, so even when it is detected early, we don’t have a treatment to change the outlook,” he told BusinessWest. “But it definitely pays to protect your body from injury, control your weight, and stay active.”
Rise in STDs Among Seniors Prompts Calls for Education, Compassion

Suzanne McElroy says the proliferation of advertising promoting senior relationships comes with little education regarding the dangers of sexually transmitted diseases.
‘Do you have protection for safe sex?’
That’s certainly not an uncommon question to ask these days, given the dangers of sexually transmitted diseases (STDs) and the widespread awareness of these afflictions.
But when Suzanne McElroy asks the same question of her clients, “they look at me with this shocked expression and ask, ‘why would I need that? I’m too old to get pregnant.’”
And that’s a big part of the problem when it comes to a growing — and alarming — trend that has emerged in recent years: a surge in the number of reported STDs among what would be considered older populations, those age 50 and up. Indeed, most of these individuals are probably too old to get pregnant, but they’re definitely not too old to contract STDs and the various health issues that accompany them.
As a franchise owner of Home Instead Senior Care, based in Springfield, McElroy knows the reality of what is happening behind closed doors with her clients, who range in age from the mid-70s to over 90, and the many issues that the aging process brings. But she also knows the disturbing statistics regarding STDs in seniors.
One of the most notable published reports is the American Assoc. of Retired Persons’ “Sex, Romance, and Relationships,” released in 2010. It surveyed a nationally representative sample of middle-aged and older people about their sex lives. These are the major findings:
• Three out of 10 respondents said they had sex at least once a week, including almost half of those who were single but dating or engaged, and 36% of those who were married;
• 85% of men and 61% of women said sex was important to their quality of life; and
• Just 12% of single men and 32% of single women who were dating reported always using condoms during sex.
That last bullet point is the really disconcerting stat, said McElroy, and just one of the reasons the Centers for Disease Control and Prevention recommends that everyone be tested once for HIV, and those who engage in risky sexual behavior should add chlamydia, gonorrhea, and syphilis to their yearly screening tests.
Elaborating, McElroy said there are two myths concerning this subject. One is that seniors don’t have sex, which is untrue, and the other is that they can’t contract sexually transmitted diseases, which is equally false. “We started an initiative around seniors and STDs, and true, it was a little shocking, and some didn’t want to be associated with it because they saw it as ‘unseemly,’ but we have to dispel these myths.”
McElroy said older Americans account for a relatively small percentage of new STD diagnoses overall, and diseases in general are escalating in the Baby Boom generation (born between 1946 and 1964) because there are simply more of them. However, the rate of STD diagnosis in those ages 50 and over has doubled over the last decade, and that constituency includes a large portion of the Baby Boomers as well as what is left of the Silent (1925-1944) and GI (1905-1924) generations.
“Also, many seniors may have married at, say, 19, and never had any other partners, and the only thing they know is that condoms prevent pregnancy,” McElroy continued, adding that it’s the reason her company offers a conversation-starter booklet called The 40/70 Rule, designed to stimulate dialogue between seniors and their children on a host of issues, including sex (more on that later).
Leslie Kayan, Healthy Aging Program coordinator at the Franklin County Home Care Corp., is a strong supporter of any conversation that opens seniors up to talking about sexuality. As a community health educator, she’s taught sex education to teens, parents, teachers, church leaders, and healthcare providers.
A Baby Boomer like McElroy, Kayan grew up during the ‘free love’ generation, a culture with an openness and knowledge about sex and STDs, which she said will carry over to her senior years. “But anyone who is older than I am is extremely unlikely to ever have had any formal sexuality education,” she said. “Many of them have been married for years, and now they are widowed and out there, at risk for the first time. And safe sex isn’t even on their radar.”
“If you look at sexuality as part of the human condition from puberty till the day we die, it just doesn’t stop,” McElroy added. “It goes through cycles, but it doesn’t stop just because we reach a certain age.”
McElroy pointed to the proliferation of senior online-dating services like www.ourtime.com, www.seniorpeoplemeet.com, and www.findseniorsonly.com; the enormous revenues for erectile-dysfunction (ED) drugs like Pfizer’s Viagra ($2.5 billion in 2012) and Eli Lilly’s Cialis ($1.93 billion in 2012); and the growth in senior and assisted-living facilities that promote socialization. The messages are tantalizing, with little education to go with them, she said.
Don’t Sleep on This Problem
McElroy has 35 employees who are fully trained in all aspects of non-medical care of seniors. To keep that training up to date and relevant, she does extensive research into a variety of subjects, including sex and the older populations.
And in many national publications that have addressed that topic, she’s seen the words ‘seniors’ and ‘frisky’ together in the same sentence, and this juxtaposition does not amuse her.
“How demeaning that readers are totally picturing two white-haired people having ‘fun,’” she said in a voice tinged with a mix of anger and frustration. “How about two white-haired people who are lonely because they lost their spouse?”

Dr. Stephen Levine says the issue of STDs is far from the surface, and it’s usually a difficult subject for seniors to bring up with family members.
“Maybe it’s romance and maybe they’re just ‘hooking up,’ but it’s not something that is funny or temporary, and it’s certainly not something that is perverse or wrong.”
McElroy’s staff does not diagnose, but rather observes any minute changes in clients like variations in appetite, urination, odors, rashes, etc., that may suggest further investigation by a doctor. According to McElroy, the biggest issue that seniors face is how the outside world sees them. It’s the widespread assumption that they don’t have sex that she said is dangerous.
“Because there is no talk about it, no education, there’s a lot of embarrassment,” she told BusinessWest. “Children will talk about healthcare proxies and living wills, and whether dad can still drive, but don’t think about asking dad about his dating or sex life now that mom is gone.”
Dr. Stephen Levine, who has practiced since 1979 in his Holyoke-based family practice and is affiliated with Holyoke Medical Center, agrees.
“The issue of STDs is far from the surface, and it’s usually the last thing that’s brought up,” he said. “It’s not something that can be allowed to be mistaken or overlooked, and needs to be discussed with the practitioner who is seeing the individual.”
Routinely, said Levine, his elderly patients have questions about physical changes that come with age and ask about ED treatments or lubrication for dryness, albeit somewhat indirectly. “A woman or a man may ask, ‘is there anything you have that can help me?’ and they know what they’re talking about, and I know what they’re talking about, and then the discussion goes in the direction of things that can be helpful, so it’s definitely on the majority of seniors’ minds that I see.”
Times are different, Levine went on, because the advent of ED drugs like Viagra for men and estrogen creams for women over the past decade has solved some of the issues of sex and aging. Now, with medical intervention, seniors are able to perform physically, with little effort, via a ‘little blue pill,’ a tube of cream, or hormone replacement therapy (HRT).
But the conversation has to start somewhere for these seniors when it comes to new sexual partners.
“Having sexual relationships is normal, expected, and OK, but it’s clear that this group is exposing one another to the possibility of STD risks,” said Levine. “Bottom line, at the start of a life-changing situation like a new relationship, testing for everything one can think of that could be transmitted sexually is a good starting point.”
Ignoring the threat of STDs, especially if they go undiagnosed, can be detrimental, Levine said, because several types of STDs can be harbored without symptoms, including syphilis, chlamydia, HIV, and hepatitis B. Syphilis, in later stages, he explained, could cause dementia, which brings up one of the difficult issues in diagnosing STDs in the elderly: many STD symptoms are similar to the normal aspects of aging.
McElroy admitted that some of her clients who normally have issues with urinating — very common in older ages — would never identify that issue as a symptom of an STD, yet it could be one.
Elaborating, Levine added, “if something doesn’t appear to be anything other than a typical aging problem, the patient will probably have no intention of being tested, but they could be infected and unknowingly be spreading infection to one or multiple partners.”
Conversation Starters
Sherill Pineda, president of Care @ Home in East Longmeadow, has become very familiar with both the concept that seniors need a healthy sex life, and the issues related to STDs.
She started a volunteer Zumba dance group for seniors called Groove and Learn, which offers exercise as just one way to stave off Alzheimer’s disease, but to also learn about other aging issues. At a certain point, the more than 25 participants, mostly senior women, wanted to talk about sex, and Pineda realized there was a definite need for more openness and awareness regarding seniors and their inability, for whatever reason, to find answers for themselves. She also realized that awareness had to spread to the senior healthcare community, which was not nearly as open as it should be, for all the other seniors in the Western Mass. region.
Last May, Pineda staged a seminar called “Never Too Old for Love” at the Western Mass. Eldercare Conference at Holyoke Community College. The symposium, crafted for nurses, social workers, and the public, drew more than 350 people, and 66 of them were seniors. (This year’s event will be held on May 29).
Pineda explained that depression is a big issue with many of her clients, largely due to the loneliness and isolation that seniors feel, especially after losing a spouse. “When I talk about ‘Never Too Old for Love,’ it’s not purely about sex; some people just want companionship, and wherever that leads, that’s their private business. As healthcare professionals, we need to be mindful about what is causing depression and other unusual changes in seniors. They are still longing for the one-on-one emotional needs and the physical aspect of it, and they’re just like us; they don’t think of themselves as old.”
Pineda has found that seniors typically won’t talk about their sex lives with their grown children, “but they are more than willing to open up to healthcare professionals, because sometimes their kids will say, ‘you’re too old for that.’”
McElroy agreed, noting that Home Instead has a resource called The 40/70 Rule, a booklet that contains suggested conversation starters concerning myriad issues in the aging process. “It means that if you’re 40, and your parents are 70, then conversations about all sorts of things should start happening.”
She said the publication has realistic ways of opening that door to at least promote a conversation between a senior and his or her physician.
Her best advice for the children of seniors, their caregivers, and doctors is to not assume anything. Financial issues, end-of-life wishes, questions or concerns about sex … no one knows unless they ask, or at least open up the opportunity for real discussion.
Spread the Word
Research, news articles, education on the part of healthcare providers, and acceptance within immediate families is what McElroy, Kayan, Pineda, and Levine say will help remove the barriers to talking openly about seniors and their sexuality.
McElroy even sees this STD issue as a trend that will likely evolve over the next decade in the form of a welcome decline in prevalence because the more open-minded individuals in their 50s, 60s and early 70s have already integrated the Internet into their lives from their work life, and information and more education will make a huge difference in their knowledge of STDs and the concept of healthy sex.
“It’s all about respect and dignity,” she said, “which dictates that, if something isn’t hurting someone, I don’t care how old you are, you should be allowed to participate in it, safely.”
Elizabeth Taras can be reached at [email protected]