Health Care
Hospice Care Comforts, Supports Memory-care Patients

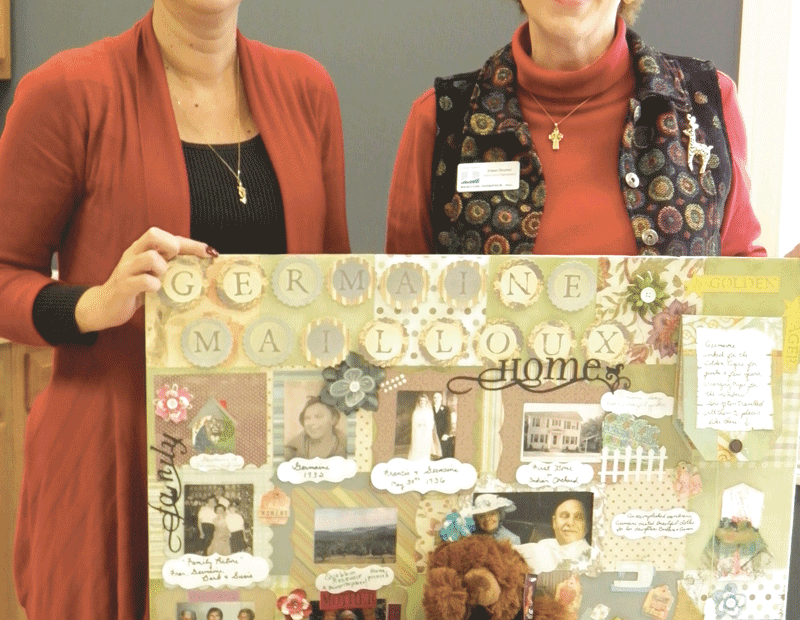
Lisa Adams (left) and Eileen Drumm show off some off the sensory ‘tools’ Beacon uses to stimulate memory in people with advanced stages of dementia.
Maureen Groden wants to dispel one of the stigmas of hospice care — the belief that it’s only for people in their last weeks of life.
“That’s a myth,” said Groden, hospice and palliative care manager for the VNA Hospice of Cooley Dickinson Inc. Take, for example, the benefits of hospice care for patients with Alzheimer’s disease.
That devastating condition robs people of their memory and ability to function while they are still alive. More than 5 million people have the disease, and the incidence of other types of dementia is on the rise. However, while many patients with a terminal diagnosis for dementia qualify for hospice care, few families seek this help.
“People lack information about what makes someone eligible,” Groden said. “There are also misconceptions about we do, which includes helping families make difficult decisions. There are many services available that people don’t know about, and families dealing with dementia need a tremendous amount of support and information.
“It’s important for them to get an early referral before the situation becomes acute,” she continued. “But people don’t know when to have this conversation, even though we do informational visits.”
Eileen Drumm, hospice service representative for Beacon Hospice Inc., echoed that assertion.
“When people hear the word ‘hospice,’ they think the person is giving up,” she said. “The biggest myth is that hospice only provides care when a person has hours or days left to live. The reason the myth exists is because so many people wait until close to the end to utilize the benefit. The word ‘terminal’ makes people freak out, but the person may have six, 12, or 18 months left to live.”
Reports from the National Hospice and Palliative Care Organization show the median length of hospice service was 21 days in 2009. However, people who receive it earlier live an average of a month longer than similar patients, and the care helps significantly with symptoms.
Hospice also offers help 24 hours a day, which is important. “People can call us at 3 a.m. if their loved one is in pain or having a hard time breathing, and our nurse will go out and visit them. We also give families a comfort kit which contains medication to control nausea or agitation,” said Joanne Schlunk, director of Mercy Hospice.
Hospice care is provided by a team that typically includes a physician/medical director, nurses, nurse’s aides, personal-care attendants, social workers, chaplains, and volunteers. In addition, the government mandates that hospice programs offer up to 13 months of bereavement support. The care is holistic and focuses on the person’s life and interests before the dementia set in, as well as their current condition.
Since dementia is a disease that progresses slowly, families become accustomed to making difficult decisions and don’t usually seek help until the situation escalates to crisis proportions. This, however, doesn’t have to be the case.
Difficult Decisions
Schlunk said patients with dementia range from those for whom it is a primary diagnosis to people whose memory loss is caused by a stroke, Parkinson’s disease, or other health issues.
Groden agreed, adding that it’s unusual for a person in their 70s or 80s to have only one disease, because health problems such as diabetes, hypertension, heart disease, and emphysema are common. But in order for an individual to qualify for hospice with a diagnosis of dementia, he or she must require significant help with daily activities, be disoriented, exhibit significant memory loss, and have approximately six months to live, assuming that the disease follows its natural course.
“People have to be pretty compromised,” she said, adding that the ability to perform daily activities does not pertain to other terminal diagnoses. “But there is a lot we can do to help. The services we provide are individualized. Everyone is unique, and although people may have the same diagnosis, there is no formula. But we can educate family members about what is normal.”
In addition, hospice providers can help families decide if they want their loved one to continue to have bloodwork or other tests for conditions that can’t be cured. That’s important because the tests can be uncomfortable, and frequent hospital visits affect the quality of life the person has left.
“You have to consider the toll it will take on the person,” Groden said. “If the person has advanced dementia and is in an ambulance, they will have no idea of where they are going. It’s not about denying people care; it’s looking at what is important to their quality of life.”
Many families don’t know they have the right to make such choices and aren’t familiar with other measures that could bring their loved one comfort. “Aggressive care doesn’t always translate into length and quality of life,” she explained. “Dignity is very, very important, and is a huge part of providing humane care. You have to really believe that each individual is a unique and important person regardless of the behavior he or she is exhibiting.”
The approach used to treat advanced dementia today is to allow people to exist in the time frame they believe they are living in, without trying to bring them back to reality. “Our goal is to make sure they are safe and their dignity is upheld. We also focus on who the individual is,” Groden said, adding that knowing a person’s interests can be helpful. “We have a volunteer who is bringing her singing group to sing with a patient in a nursing home who used to love to sing herself,” she said. “And another patient loved animals, so a volunteer brings her dog to visit.”
Advanced dementia can cause agitation and behaviorial changes. But it’s a mistake to simply attribute yelling to the disease, because the behavior may be caused by pain. A pain assessment is critical for patients, Groden said, explaining that conditions such as advanced arthritis or spinal stenosis can be helped with a good mattress and medication, while squirming in a chair may be related to bed sores or a skin condition. “Don’t assume the person is yelling just because they have dementia. You can almost always make things better.”
Necessary Measures
Decisions in the end stage of life can include whether to have a feeding tube inserted into the stomach, which carries risks and benefits and can prolong or shorten life. This measure becomes necessary because dementia can cause the muscles of the throat to stop working properly. And although food keeps people alive, eating and/or a feeding tube can result in aspiration pneumonia, which occurs if food ends up in the lungs instead of the stomach. “It’s a hard decision,” Schlunk said.
Groden agrees and says food is equated with nurturing, so when someone can’t eat, it weighs heavily on people’s hearts, which is another reason why it is important to help the patient stay independent as long as possible.
“Decisions have to be made again and again, and it’s really hard for families because there are so many periods during the course of the disease when they have to do research, especially if the person is confined to bed, is weak, and has lost a lot of function,” Schlunk said. “Caregiving can lead to exhaustion, so we help families at different stages of the decline.”
In many cases, family meetings are needed. “You need facts to make good decisions, and also need to know what the expectations are for your loved one,” Schlunk said. “And everyone needs a chance to be heard. Although everyone in the family may love the person, a caregiver who lives with the patient may have a more difficult time letting go.”
Resentment and other related emotions can arise when siblings who live far away express strong opinions to caregivers, who often feel abandoned and are left to deal with the agitation and loss of recognition that often occurs as dementia advances. “But people [with dementia] still have moments of lucidity and may say something that has such profound meaning that their loved one knows the connection is still there,” she added.
Hospice volunteers can provide a supportive presence. They often read to the person, play music, or simply sit and talk or hold the patient’s hand. “We all have an inner need for connection, and having the sense that someone is nearby helps people feel less lonely. They are still having inner experiences, and when you don’t understand what is happening in your environment, it can be very scary,” Schlunk said.
Drumm agrees. “Family members have expectations, and when they are not met, they become discouraged. But the purpose of a visit should be to have their loved one feel connected instead of being isolated in a room. The person takes in their environment even though they may not recognize people, so one of our goals in hospice is to educate families and help them find new ways of connecting.”
They also try to keep the environment soothing. “It’s important to prevent the patient from becoming overstimulated. Even the sound of the shower can be frightening because, when a person loses their memory, they don’t have the context to understand noises,” Groden said.
Bereavement support can be valuable, and Schlunk said primary caregivers may suffer the loss of the person they loved as well as the loss of their role. “They may begin to second-guess decisions they made. Sometimes there is a lot of regret.”
Inside the Mind
Beacon is affiliated with Amedisys, which is the largest home health care company in the country, and its goal is to provide a continuum of care with seamless change as the end of life approaches.
Director of Operations Lisa Adams said typical changes caused by advanced dementia include the loss of speech and the ability to walk, weight loss despite average nutrition, and pneumonia and infections, which set in as the body loses its ability to function normally.
“A person may take an hour and a half to eat one meal,” she said, adding that a hospice provider will have the patience to sit with the person and give them that time, rather than assuming they aren’t hungry.
Beacon created a program called Deep Harbors for Dementia, which contains a number of measures designed to provide comfort. “We work to create a connection between the patient, their loved ones, and staff members who work with them to preserve the patient’s dignity,” Drumm said. “Family members often pull away from visiting the person, as they don’t like to watch them get worse, which upsets patients even if they can’t express it.”
She added that touch is very important, and although family members may wonder why they should visit if their loved one doesn’t know who they are, “on some level, they do know you. If you take their hand, they will know you care about them,” she said, explaining that small things such as massaging a patient’s hand can bring them comfort. “The problem is that families look to the person to be who they were. But the disease is not their fault, and they are still human and very much alive.”
Beacon’s work with the Berklee School of Music revealed that tunes people with dementia enjoyed in their teens and 20s can elicit a positive response as the disease progresses, so its program includes creating a compact disc of music for every patient. “One lady we cared for would sing along to every word from ‘Love Me Tender’ by Elvis,” Drumm said. “It was incredible to see, and helped her family realize that her spirit was still there and there was still memory in her body.”
They also create a Chart of Life after interviewing family members. “One day a woman looked at it, pointed to her bridal picture, then touched her wedding ring,” Adams said, adding that it meant the world to her family.
Their ‘tool kit’ also includes a teddy bear, and although it’s important to avoid treating patients with dementia like children, having something soft to touch can be comforting.
“We honor people, validate them, and meet them where they are. Our goal is to help families enter their loved one’s world, since the person can no longer enter theirs,” Drumm said. “It’s all about love.”
They also give patients a cloth activity pad. One side is soft and fuzzy, while the reverse side contains large buttons, pockets, zippers, and a compartment to hold photos. “It’s good for people who worked with their hands, as it keeps them busy,” she said.
Early Intervention
Drumm said it’s never too early to call and inquire about hospice care, as providers can refer families to other services they may need.
“Hospice care is for the whole family,” she said. “The end stage of the disease can cause conflict, which amplifies the family dynamic as emotions run so high.
“Our philosophy,” she added, “is that we want people to have a peaceful death. We don’t want anyone taking worry and anxiety from this life to the next, so anything we can do to help ease the heart, mind, and spirit of the dying person is important.”

Mercy’s Expanded, Renovated ER Is a Statistical Success

Dr. Louis Durkin says Mercy’s updated ER successfully addresses issues of flow and flexibility, improving the department’s overall performance.
There were and are many goals and ambitions behind the $1.3 million expansion and renovation of Mercy Medical Center’s Emergency Department, but those two words pretty much tell the story, said Dr. Louis Durkin.
He’s the medical director for the Department of Emergency Medicine at Mercy, and while he didn’t actually design the ER improvements, he worked hand-in-hand with the architect to blueprint a facility designed to enable the department to move patients in and out more quickly (the ‘flow’ part of the equation), due in large part to space that can be used for many different purposes and to treat patients with various levels of emergencies (there’s the flexibility).
Ready for business starting early this fall, the expanded and renovated ER is already yielding improvement in some of many barometers used to track performance in the ER, said Durkin, citing both the “door-to-provider” measure — the medical center is now averaging under 30 minutes, the industry benchmark — and the stat known as “door to door,” which is now under four hours, another industry standard.
“For fast-track patients, it’s usually under 90 minutes,” he said, referring to those with less-serious issues. “But for our total population, which includes the patients that are admitted to the hospital with large workups, there is now a turn-around of under four hours, which is pretty good.”
Meanwhile, there’s also been improvement in another measure, the so-called “left without treatment” measure,” which, as the name suggests, denotes people who have left the ER for one reason or another — the wait was too long or the simply changed their mind, for example. At Mercy, that number has come down from 6% to 2% over the past several months.
The renovated ER passed a significant test during the recent late-October snowstorm, said Durkin, noting that resulting power outages taxed the facility and its personnel because many patients couldn’t be discharged to homes without power. And it will get another test in the flu season due to start later this month.
But he is confident the facility will bear up to those challenges because of the detail that went into the design, and also because of that level of flexibility, which enables the ER team to continually tweak and improve the facility and its operations.
Durkin told BusinessWest that the enhancements to the ER have been in the planning stages for more than two years now, and were made necessary by escalating numbers that were not an aberration but a trend expected to continue for many years.
Elaborating, he said that ER volume, which was averaging just over 70,000 several years ago, has been escalating steadily, peaking at 79,000 in 2009, and averaging more than 75,000 the past few years. The reasons for upward movement of the needle are many, he explained, citing two important trends — a significant rise in the number of people who have health care insurance (thanks to reform measures in the Bay State) coupled with stagnancy in the number of primary care physicians — as primary drivers.
“You have more people with insurance, but you have the same number of primary care physicians,” he said, adding that the bottom-line result is more visits to all ERs, and especially Mercy’s, one of the busiest in the state.
In response to the trend and its impact on some of the statistics referenced earlier, Mercy blueprinted a project that would increase the number of ER beds from 32 to 43, said Durkin, adding that this would yield significant improvement in another industry barometer for emergency departments. This would be the one using an official target of one bed for every 1,200 patient visits per year.
Mercy was well above 2,000 per bed before the expansion, and is now much closer to the industry goal, Durkin continued, adding that it is not only the number of beds that is improving overall statistical performance, but also that aforementioned flexibility in how they can be used.
To illustrate, Durkin provided a quick tour of the new ER, which is the result of a project that involved expansion, consolidation, renovation, and modernization. There are now five color-coded pods, or areas designated for specific types of patients. These include the so-called fast-track, or less-serious cases; acute cases (those more serious); and those involving patients with behavioral-health or substance-abuse issues.
Before, the ER had just one bed designated for behavioral-health-related cases, he said, adding that capacity for such cases has quadrupled, and even those expanded facilities are usually at or near capacity.
While each pod has a specific use, there is a large amount of flexibility that is part and parcel to emergency-room operations, and the new ER provides more of that commodity.
“The ideal flexibility comes when any patient can be seen in any bed, as opposed to having specialized beds and specialized rooms,” he explained. “We still need to have those, in that we have acute-resuscitation pods, but for the most part, we have more flexibility; if we start getting a higher number of more-acute patients, we can treat them in the fast-track area, and vice-versa.
“Soon, we’ll be able to treat almost any patient anywhere in the department no matter how acute they are,” he continued, “and that’s important, because most bottlenecks occur when you have specific rooms that you can only use for suture, for example. The ratio of acute to not-so-acute patients changes from day to day and hour to hour, so you have to be ready and make sure you can evenly distribute the workload.”
George O’Brien can be reached at [email protected]
Most Sports-related Neck and Back Injuries Are Preventable
Dr. Julio Martinez-Silvestrini calls them “the terrible toos.”
“People do too much, too fast, too soon,” said the sports medicine physician from Baystate Rehabilitation Care in East Longmeadow, as he talked about how and why sports-related injuries to the spine occur.
“If people followed simple rules, they could avoid most injures. But getting in shape takes time, and people are impatient. As soon as the snow melts every year, golfers go out and play 18 holes without stretching. And someone who has never run before will decide to run a marathon, put their sneakers on, and run two miles the first day,” he said, adding that such individuals usually end up getting hurt.
Dr. Charles Mick agrees. “If you want to lift weights, don’t try to lift 250 pounds the first day,” said the orthopedic surgeon from Pioneer Spine and Sports Physicians in Northampton. “Athletes want to maximize their ability, but they need to do it gradually with common-sense training.”
But many people make the wrong choices. In addition, some sports injuries cannot be avoided. As a result, physicians see adolescents and adults who have injured their neck and/or back playing sports. Their conditions range from muscle strains and sprains to ruptured discs and, in rare cases, spinal-cord damage, which can result in paralysis or even death.
The injuries occur from participation in a wide variety of activities, which include golf, running, football, baseball, BMX biking, martial arts, cheerleading, lacrosse, diving, horseback riding, car racing, surfing, and more.
“Most of the time, back injuries are not related to an acute event,” Martinez-Silvestrini said. “They result from overuse and repetitive movements using bad body mechanics.”
Anatomy Lesson
Martinez-Silvestrini says the back can be divided into three parts: the cervical or neck region, the mid-thoracic spine, and the lower or lumbar spine.
In general, muscle strains are the most common type of injury. “At some point, almost every athlete strains a muscle,” Mick said. “Sore backs are common, and aches and pains are part of getting stronger.”
However, Dr. Christopher Comey of New England Neurosurgical Associates in Springfield says it’s not unusual to see patients with injuries that range from nerve irritation to cervical spinal fractures.
“Lumbar or lower back strain usually responds to pain medication, restriction of activity, and anti-inflammatory medication. Longer-lasting injuries can involve pinched nerves, which can happen when a disc is herniated and a piece of it lodges against the nerve. The pain can start out in the back and, several days later, travel down the leg. But only 10% of patients with these conditions require surgery,” he said. “The majority respond to physical therapy, rest, and, on occasion, cortisone injections.”
The most common injury to the neck is whiplash. “It can happen in any sport where the person is moving at high velocity; if a football player is tackled in the chest, his neck continues to move forward, which stretches all of the ligaments and muscles that support the cervical spine,” Martinez-Silvestrini said. “Once you get to the point of maximum deformity, there is a recoil mechanism, and the neck goes backward.
“Sometimes, it overcorrects and bounces back and forth,” he continued. “The opposite happens when someone is tackled from the back. Their neck snaps backward, which stretches all of the front neck muscles because the head is moving at a different velocity than the trunk of the body.”
In most cases, whiplash results in nothing more than a stiff neck, which improves with rest. “The way to differentiate between a mild sprain versus a more serious one is pain that doesn’t improve with rest, or tingling or numbness,” said Martinez-Silvestrini. “In more severe cases, there may be weakness, walking difficulty, or problems with bowel or bladder control.”
A common football and wrestling injury is called a ‘stinger’ or ‘burner’ because it causes sudden pain and/or numbness and tingling that lasts for a few seconds and feels similar to hitting the ‘funny bone.’ It results from overstretching the brachial plexus network of nerve fibers that run from the neck to the arm.
Mick says stingers can be frightening, but are usually not dangerous. However, in rare instances there can be permanent nerve damage, and symptoms should not be ignored if the athlete has another episode during play.
Injuries to the thoracic vertebrae in the back are typically mild, since the rib cage provides protection and stability. However, if and when they do occur, they can result in damage to the spinal cord.
But lower back pain is the complaint that sends most people to their doctor. And although many people ignore it, Comey said chronic low back pain in young athletes should be taken seriously.
“There is a tendency to think, ‘it’s a kid, so what could possibly be wrong?’ But I have seen children who have developed stress fractures in the lower spine,” Comey told HCN. “If they’re recognized early, they can usually be treated with non-surgical means, including external bone stimulators that encourage bone growth.”
However, if a stress fracture in a young person goes untreated, they can develop slippage of the spine, or spondylolthesis, which typically occurs when the L5 bone slips out of the proper position and slides forward on the first bone in the pelvis or sacrum, which causes back and leg pain.
Braces are sometimes used to treat stress fractures in young athletes, and they may be able to return to playing sports after the fracture heals, Comey said.
But in many cases, the fracture never heals, and although the pain subsides, it can reoccur if the person returns to play. “I’ve had several UMass varsity football players who were unable to play again,” Mick said.
Prevention Matters
Correct posture, proper equipment, maintaining flexibility, and overall conditioning can go a long way toward reducing neck and back injuries, experts say.
“People need to be fit to play a sport, rather than playing sports to be fit,” Martinez-Silvestrini said. “Three major elements that are important are flexibility, strength, and good aerobic capacity.”
Mick agrees. “A sports program needs to be balanced,” he said. “Sometimes football players will only do strength training and not work on balance, which is very important. And when people think about baseball, they think about the shoulder. But if someone wants to throw a pitch at 90 mph, they need to use their leg, trunk and back muscles. So if they just exercise their shoulder and arm muscles, they may injure their back when they are throwing fastballs.”
Golf is another sport where posture is critical. “When someone wants to pick up a golf ball, they should bend down or use a golfer’s reach,” Martinez-Silvestrini said. He demonstrated the move by leaning forward while keeping his back straight and reaching out with one hand while extending the opposite leg.
Comey says golf is not bad for the spine, but people with low back problems need to warm up and do some stretching before they begin to play. He recommends people visit www.spineuniverse.com to learn helpful exercises.
Physical therapy can be useful after an injury, and sessions with an athletic trainer or coach can make a difference after initial healing takes place. “A trainer can create a program that focuses on strength, endurance, balance, and coordination,” Mick said.
However, some people are unable to return to the sport that led to their injury, especially if their lower back pain is caused by degenerative changes.
“Distance running can be very difficult on the lower back due to the constant pounding transmitted to the spine with each step,” Comey explained. “Pain can come from discs which no longer function as shock absorbers. They literally wear out, which is no different than wearing out a hip or knee.”
Worthwhile Pastime
The bottom line is that most spinal sports injuries are mild and don’t cause permanent damage. “If pain goes away within a day or two and is fairly mild, there is no need to get excited,” Mick said. “But it does need to be evaluated if it is severe, keeps coming back, or doesn’t go away.”
Comey agrees and says 90% of people develop debilitating back pain at some point in their life.
But the risk of hurting one’s back or neck is not a reason to avoid sports, Mick said. “The benefits of regular exercise and participation in sports far outweigh the risk of injury.”
Baystate’s New COO Puts the Focus on Quality and Value
Greg Harb was asked about the job description for the title on his business card — chief operating officer/executive vice president at Baystate Health, a newly created position at the region’s largest health network.
He said part of it is creating an operational road map for this system, which has a wide array of facilities stretched across three counties and more than 10,000 employees, a task he says involves everyone at Baystate Health. “But it’s more about keeping everyone on course — following that map and getting to where we want to go.”
Elaborating, he said that it’s one thing to have a plan or a multi-faceted strategy for providing quality care in an increasingly challenging environment for all providers (and Baystate has one, which he would expand on in great detail), and it’s quite another to properly execute that plan. And in many ways, his job description comes down to leading, or enabling, effective execution.
“I’m working closely with physician leaders, and also interacting frequently with front-line co-workers,” he said by way of explaining his role within the system. “We’ll have open forums on a regular basis, and I’m also working with the leaders of our different operating entities — the hospitals, the physician practices, our home health and visiting nurses associations — to make sure we’re executing those system objectives and system strategies.
“We’re constantly spending time evaluating our strategies,” he continued, making use of the collective ‘we,’ as he would repeatedly as he talked with BusinessWest, “and ensuring that we’ve got the right tactics to execute those strategies.”
And, as he said, there are many components to the system’s strategic plan. He identified five core strategic objectives, all in support of the integrated health network he says is the model of the future:
• A focus on quality of care provided;
• “Financial stewardship of this community resource”;
• Ensuring that the system is providing innovation in how it provides care;
• Commitment to academic endeavors; “we want to continue to educate health care professionals in the future”; and
• Ensuring that the system “has the most talented group of co-workers in this part of the country.”
Summing all that up, while also condensing his own job description even further, he said it comes down to that simple (yet also exceedingly complex) term ‘value’ and how to provide it in everything the system does.
For this issue, BusinessWest talked at length with Harb about his new assignment at Baystate Health, the many components of his job description, and that all-important focus on value.
Background Check
Harb comes to Baystate from the St. Joseph’s/Candler (SJC) Health System in Savannah, Ga., where he took the same title he has now: chief operating officer. Prior to that, he was COO and executive vice president of the Baptist Health System of East Tennessee, and held similar positions at Valley Baptist Health System in Harlington, Texas, and Memorial Hermann Healthcare System in Houston.
Like Baystate, SJC is an integrated system with a number of components, including two hospitals (St. Joseph’s and Candler, each with roughly 300 beds), a home-health component, the Lewis Cancer and Research Pavilion, and many other programs.
Harb listed a number of accomplishments from his five-year stint at SJC, including an improvement in net operating income from $336,516 in FY 2007 to $3.1 million in FY 2008 and $8.6 million in FY 2010; development and implementation of a strategy that decreaed premium pay 30% compared to the same period the prior year, resulting in a $4.4 million annual savings; decreasing labor as a percentage of net patient revenue from 44.6% in FY 2005 to 39.9% in FY 2010; work with the system’s board to establish a ‘collaborative’ with a competing health care system, with the primary objective of reducing supply cost; and co-leadership of an enterprise-wide “patient throughput initiative,” which resulted in a 0.4-day reduction in average length of stay at each hospital.
He told BusinessWest that recruiters brought him into the search for a COO at Baystate last fall, and he was attracted by the prospect of working with others there to lead the system through a challenging period of transition for all providers.
“What was most appealing about Baystate is that this is truly one of those integrated regional health networks,” he explained, “where you’ve got Health New England as the payer partner, comprehensive and regionally distributed acute-care hospitals, an integrated, multi-specialty physician practice within the system, all the outpatient services, and parts of the continuum of health with home care and hospice,” he explained. “So Baystate is very well-positioned to really lead the transformation of care, and that was very exciting to me as a professional.”
During the interview process, he said he had the opportunity to meet with Baystate leadership, including CEO Mark Tolosky, whom Harb described as “dynamic,” as well as board members, and came away impressed with the common vision and the basic approach to achieving it.
“There was singularity in terms of their focus on wanting to be that integrated regional system and trying to position Baystate to really change the way care is delivered,” he explained.
Upon arriving in March, Harb said he spent a considerable amount of time acclimating himself to the Baystate system and understanding the dynamics of the many moving parts within the delivery network.
When asked what he took away from that acclimation process and the many forums he had with administrators, physicians, and employees at every level, he said it was the sense that everyone is pulling in the same direction.
“There’s a real commitment to Baystate Health’s strategies, a commitment to the execution of those initiatives, and a real positive outlook that, if we do execute those strategies, we’ll continue to be a leader in Western Massachusetts,” he said. “There was a positive outlook that we’re well-positioned as a system, but that doesn’t mean that there weren’t or aren’t significant challenges facing Baystate and everyone else in health care.”
Care Package
Which brings him back to the five core strategic objectives he mentioned earlier, and how they are all integral to that process of providing value and enabling systems to effectively serve the public when the costs of providing services (especially in the case of Medicaid and Medicare) are not fully reimbursed by payers.
Starting with that term, or philosophy, of quality, he said that it comes in three areas: clinical — the outcomes provided — as well as patient experience, which Harb described as a “core deliverable,” and access. “We want to ensure that our community has access to our physician practices, acute-care services, as well as our outpatient services.”
And a big component in the effort to deliver quality is transparency, he told BusinessWest, adding that the system posts all clinical outcomes on its Web site.
Regarding financial stewardship, Harb said a key part of this strategic initiative is removing waste from the system in order to provide care in the most cost-efficient manner. As part of that effort, the system started down what he called a “lean journey” nearly 18 months ago, and now applies lean practices in a number of departments, leading to significant gains in efficiency and plans to expand the program.
Meanwhile, the system, which has undergone a large reduction in force (185 positions were eliminated in late June), has also focused on non-labor expenses, such as costs within the supply chain, he continued, and has managed to reduce expenses by roughly $40 million to $50 million over the past several years. “We’re constantly looking at ways to remove waste without compromising quality,” he explained, adding that such efforts are helping Baystate toward its three-year goal of breaking even on Medicare services (which constitute a large percentage of total volume within the system).
Innovation in the delivery of services plays a part in both the achievement of quality and financial stewardship, he continued, citing as one example, the advent of patient-centered medical homes (the system has 16 of them), a relatively new model of the organization of primary care. It involves an individual’s primary-care physician and family and focuses on care needs, including prevention and wellness.
“These homes, which coordinate care across the entire continuum, are a real innovation and an opportunity to improve the way in which we provide care,” Harb said, adding that another key to Baystate’s success quotient is recruitment of top talent across the board.
“We need to make sure that we recruit, retain, and develop the best physicians, the best nurses … all parts of our delivery system,” he said. “We have an aging workforce, so the constant challenge of recruiting and retaining our caregivers is something we spend a lot of time on. And we understand that this is at the core of all that we provide; the people — the team — are the most important element in the process.”
And the ongoing task of proper execution of strategic initiatives is a total team effort, he went on, summing up the many financial and operational challenges facing providers by saying that they must continue to “appropriately redesign care and remove waste, but not impact quality of care.”
Elaborating on this redesign process, he said it involves reduction, or elimination, of the fragmentation process in health care today, and the creation of truly integrated systems. This is a large component of Harb’s assignment, and one of the many motivations behind the $250 million Hospital of the Future expansion now taking shape on the Baystate campus.
“One of the core parts of my responsibility is seeing that we’re truly integrating our care,” he said, “and that we’re not just approaching it from a hospital perspective, or from a physician-practice perspective, or a post-acute perspective, but making sure that we are truly coordinating that across the system.”
Bottom Line
When asked how he would evaluate his level of success in his new position, Harb said there would be a number of effective measures.
“Are we hitting our quality metrics? Are we hitting our patient-experience metrics? Are we performing well financially? Are we recruiting and retaining our talent? Are our co-worker engagement scores improving? It’s very much based on how we perform against the measured objectives of our system,” he explained.
In more simple terms, though, he’ll be successful if he can keep the system on course, able to follow that roadmap for progress in a changing health care landscape, and, in a word, execute.

The Employment Outlook Remains Strong in Health Care
 In many respects, the phrase ‘jobless recovery’ still applies to the landscape in Western Mass. But one key sector where that term doesn’t fit, or at least to the same degree, is health care. Indeed, shortages exist in many specialities, and hiring remains steady across the field. This situation presents opportunities for job seekers and career changers, but many positions require degress and completion of challenging programs.
In many respects, the phrase ‘jobless recovery’ still applies to the landscape in Western Mass. But one key sector where that term doesn’t fit, or at least to the same degree, is health care. Indeed, shortages exist in many specialities, and hiring remains steady across the field. This situation presents opportunities for job seekers and career changers, but many positions require degress and completion of challenging programs.
In the midst of a still-sluggish economy that, overall, is adding jobs at a frustratingly slow pace, Cathy Dow-Royer paints a significantly rosier picture.
“We’re seeing an increase in the number of students coming through,” said Dow-Royer, director of the Occupational Therapy program at American International College. “A lot of students are interested in medical fields like occupational therapy, and they’re seeing no problems getting jobs at all.”
Overall employment trends are packed with good news for the health care sector. According to the U.S. Bureau of Labor Statistics, about 26% of all new jobs created by the nation’s economy between 2008 and 2018 will be in health care and social assistance — a broad category encompassing hospitals, nursing and residential-care facilities, and individual and family social services.
Those fields overall are expected to expand by about 24% over that 10-year period — an increase of about 4 million jobs — driven largely by an aging population and longer life expectancy in the U.S.
David Miller, dean of the School of Health Sciences and Rehabilitation Studies at Springfield College, cited data from the same report as he talked optimistically about this sector and its future. He noted that, for specialties represented in his institution’s roster of programs, the numbers are often even better — 39% for physician assistants, 37% for athletic trainers, 30% for physical therapists, 26% for occupational therapists, 21% for substance-abuse counselors, 19% for rehabilitation counselors, and 19% for speech and language pathologists.
As a result — at least in Springfield College’s case — young people mulling career options are increasingly giving health care serious consideration. “Enrollment in our [health] programs a few years ago was in the 500s, then the 600s, then the 700s, and now the 800s, so we’ve had steady, incremental growth,” Miller said.
“One of the reasons for that,” he continued, “is that prospective students and their families see that there are very good opportunities for employment on the other end — and that is, in fact, the case for 100% of our graduates, or very near that.”
Many of these programs require some clinical rotations or other field work, which exposes students and employers to each other, often greasing the tracks to a full-time job, he added. “Once they’re there, and they like the job and the employer likes them, our students are often offered employment in that setting. It’s a great opportunity for employers to work with our students and supervise them during their training.”

Cathy Dow-Royer says most graduates from programs at American International College have little trouble finding jobs in their chosen fields.
These employment success stories are being echoed across the region, in a wide variety of medical disciplines. But in many cases, job seekers must complete much more education and training than in the past, and need to be more flexible about where they want to work. But in most cases, the end result — a steady, good-paying job — is more than worth the effort and expense.
Outside the Office
According to Dow-Royer, one reason her department’s graduates are experiencing a solid hiring outlook is because occupational therapy has expanded its reach into so many areas of health care.
“Hospital outpatient rehabilitation is one area of practice, as well as prevention and chronic care management,” she said, which can include care at home, at skilled-nursing facilities, and elsewhere. “We’re working in primary care, with intensive care units, we’ll always be involved in mental health, and then there are extremity programs — working with doctors doing surgery on hands and arms, and getting people back to work again.”
Miller agreed. “To some extent, this is not necessarily hospital-based,” he said. “Some of the robustness is due to a shift away from bricks and mortar, from acute-care hospitals, into community-based settings. Home care, for instance, is projecting a 46% increase.
“There are rich opportunities — I don’t mean fiscally rich, but robust opportunities — in geriatrics,” he continued, citing the ever-advancing age of the Baby Boom generation, many of whom are living longer with chronic medical conditions than ever before. “Many of us are crossing that threshold into our 60s. People are living longer and want to be active and well and continue to work.”

Lynn Ostrowski, director of Health Programs and Community Relations at Health New England, says health insurance is just one of many fields experiencing job growth.
“Even in this economy, we have been measurably growing,” she said. “It’s been slow but steady growth, and as we have entered new lines of business and marketed a variety of products, we’re looking for a trained workforce to come in and do these jobs. It’s getting more and more specialized. Medicaid product requirements are very different from Medicare products, and so on.”
That means looking for employees with a variety of skill sets, Ostrowski explained. For instance, “we have this brand-new role today — it’s a Medciaid community outreach leader, and we have a huge need for people who are bilingual. It was very difficult for us to fill this position. It took us almost six months to find someone with some knowledge of medicine with communication skills, who could work with members, someone we could teach the plan to and have them hit the ground running.”
At a recent seminar in Springfield on health-insurance reform (see story, page 32), state Rep. Michael Finn, D-West Springfield, said lawmakers recognize a shifting of jobs across the health care landscape, and have created a workforce-development fund that helps people working in struggling health care fields to transfer into areas with healthier employment rates.
In addition, he noted the state’s chronic shortage of primary-care physicians, exacerbated by pay disparities with other specialties and the five-year-old mandate that every citizen must carry insurance, creating access issues at doctors’ offices. In response, the state is exploring options such as loan-forgiveness programs and regional-disparity payments to try to broaden the pool of medical students entering primary care.
Back to School
While opportunities in many fields are expanding, however, education requirements are increasing as well. Occupational therapy, for example, is now typically a master’s-level program, while incoming physical therapists almost universally need a doctorate today. Even careers that once required just an associate’s degree now demand a four-year track of study.
Ostrowski’s “other hat,” as she called it, is coordinator of the Health Services Administration degree program at Elms College. “I teach mostly students who have an associate’s degree in some form — it may be occupational therapy assistant, nursing assistant, physical therapy assistant, dental hygienist — but most of these jobs we’re talking about need a bachelor’s degree just to be looked at.”
However, through a partnership between Elms and Holyoke Community College, these students can complete their bachelor’s degrees in less than two years through a Saturday program, making the track ideal for students who need to work or support a family while moving toward greater career opportunity.
“The tuition is the HCC tuition structure, but they get the degree from Elms College, so it’s a great opportunity for people to come into the health care field who have only an associate’s degree, but need to get their bachelor’s degree quickly.”
“From skilled-nursing facilities to the managed-care environment to teaching hospitals to rehab facilities, there are just so many different places where people can work,” Ostroski said. “The goal of the program is to give people experience across the entire industry so they can get an idea of what role they want to have, and then prepare them to take on that role. As soon as they get that bachelor’s degree, their salary goes up significantly.”
But it’s more than salary, Miller said. For those willing to make the necessary commitment to education, the result is usually a job that’s both well-paying and personally gratifying.
“There are wonderful opportunities — good jobs with good benefits — and if you look at job satisfaction, these are people who like some control over their day, respect, and work that makes a meaningful difference in someone’s life,” he said. “These are really positive things.”
Joseph Bednar can be reached at [email protected]
A chart of the region’s behavioral health centers
Click here to download PDFBehavioralHealthCentersBW1011b
There Are Many Such Matters Involved with ‘the Long Goodbye’

Todd C. Ratner
Alzheimer’s disease, the most common form of dementia, is a physical and terminal illness that causes difficulties with memory, thinking, and behavior. It is not a normal part of aging.
According to the Alzheimer’s Assoc., there are 10 common warning signs of Alzheimer’s disease:
• Memory changes that disrupt daily life;
• Challenges in planning or solving problems;
• Difficulty completing familiar tasks;
• Confusion with time or place;
• Trouble understanding visual images and spatial relationships;
• New problems with words in speaking or writing;
• Misplacing things and losing the ability to retrace steps;
• Decreased or poor judgment;
• Withdrawal from work or social activities; and
• Changes in mood and personality.
Alzheimer’s gets worse over time; however, one advantage of a timely diagnosis is that the person living with the disease can often participate in their own estate planning. This allows them to decide who will make medical and financial decisions on their behalf in the later stages of the disease, provided, of course, that they still have the legal capacity — the level of judgment and decision-making ability — needed to sign legal estate-planning documents.
As such, it is imperative that someone diagnosed with Alzheimer’s begin making legal and financial plans as soon as possible, to the extent that they can. If there are any questions as to whether or not your loved one has the necessary legal capacity, a medical provider should be consulted.
The following should be considered immediately in the event that your loved one does not have a current or updated plan in place.
Estate Planning
Estate planning, in its most basic essence, is a process for nominating a trusted person to make medical and financial decisions and planning for the disposition of your assets upon death. Regardless of the size of your estate, there are several essential considerations.
Everyone needs a will, the most basic estate-planning document. It provides for the orderly distribution of your estate upon your death. In Massachusetts, the state has already drafted a will for you, designating that your assets pass in proportions of 50% to your spouse and 50% to your children, so if you want any customization, you’d better have an attorney draft a personalized version for you.
Another essential estate-planning tool is a health care proxy. This document allows a designated person, called a health care agent, to make health-related decisions for you if you become incapacitated and cannot make them yourself. This becomes especially prevalent when Alzheimer’s disease progresses, as your loved one will understand your wishes regarding care and end-of-life decisions.
Another critical estate planning tool is a durable power of attorney. This document gives a person called the attorney-in-fact the ability to handle your financial affairs during your lifetime when you are incapacitated. This will prevent your loved ones from having to go to court and obtain the legal right to pay your bills and handle your finances on your behalf when your disease progresses.
Estate planning is a broad term that can encompass many things, and there are more estate-planning choices available today than ever before. You may also consider various trusts to provide for the continued financial support of your family members after you lose the ability to care for them yourself.
Long-term Care Financing
While most families prefer to keep their loved one at home as long as possible, it is common for an individual with Alzheimer’s to have to go to a nursing home when family members can no longer provide the necessary round-the-clock care. Due to the characteristics of the disease, Alzheimer’s residents typically reside in nursing homes longer than other residents. Since the average cost of a nursing-home placement in Massachusetts is approximately $10,000 per month, long-term care financing is a critical component of the planning process for a loved one with Alzheimer’s disease. As such, effective planning for long-term care financing is a must to preserve your family’s assets against being drained by a nursing home.
The available options to pay for nursing-home care include private payment, long-term care insurance, and Medicaid. Private payment can quickly evaporate a lifetime of savings and significantly limit the amount passed to designated heirs, so it is generally preferred to find an alternative form of payment.
Long-term care insurance is a wonderful way to pay for a nursing home stay, but one must be insurable in order to be eligible to purchase such insurance, which precludes most people living with Alzheimer’s. It may also be expensive, thereby making it an unaffordable option.
Many people think that they can simply give away their money to family and friends freely. They often don’t understand that complicated Medicaid laws include a specific look-back period on all assets, and such transfers will delay Medicaid eligibility, requiring you or your loved one to find alternative financial resources until the waiting period is satisfied. Without proper planning, this delay could financially devastate your family, but Medicaid planning or asset preservation can be accomplished by properly transferring assets in accordance with Medicaid laws, and an estate or elder-law attorney can guide you through that process. It may be your best way to prepare for an anticipated nursing-home stay.
Even if a loved one is afflicted with Alzheimer’s disease and does not have an updated plan, it may not be too late. However, it is important to see a qualified estate-planning and elder-law attorney as soon as possible to ensure that the ever-changing and intricate laws and requirements regarding estate planning and long-term care planning are followed. Such an advisor is the best resource for determining how to effectively draft an effective estate plan that can help preserve your family’s resources.
You can be a voice and an advocate for the 5.4 million Americans living with Alzheimer’s disease. The local office of the Massachusetts/New Hampshire Chapter will be hosting events throughout the month of November to celebrate and promote awareness of the disease. Log onto alz.org/manh to find out more.
Todd C. Ratner is an estate-planning, elder-law, business, and real-estate attorney with the regional law firm Bacon Wilson, P.C. He serves as the co-chair for the Alzheimer’s Assoc. Tri-County (Hampden, Hampshire, and Franklin) Partnership and is a member of the National Academy of Elder Law Attorneys and the Estate Planning Council of Hampden County. He is also a recipient of Boston Magazine’s Super Lawyers Rising Stars distinction from 2007 to 2010; (413) 781-0560; baconwilson.com

Baystate’s Hospital of the Future Set for Spring Opening

The facade of the soon-to-be-opened expansion along Chestnut Street.
When the Hospital of the Future opens to the public in March, only about half of the newly constructed building will be usable.
But without the hundreds of thousands of square feet of shell space included in the project, Baystate Medical Center might as well dub it the hospital of today, said Stanley Hunter, project executive. And that would miss the point.
“We call it the Hospital of the Future because we’ll be able to respond to the changing needs of health care in the coming years,” he said while taking the BusinessWest on a tour of the floors that will be bustling with patients this spring.
“The building itself is 640,000 square feet, which we’re fitting out in phases,” Hunter explained. “The first phase, just under half the building, will house our Heart and Vascular Program.”

Stanley Hunter, outside what will eventually be the hospital’s new main entrance, says heart and vascular employees will start moving into the expanded space this fall.
“We’re excited that we’re on schedule,” he added. “We’ve always had that [March] date in mind, so it’s exciting that we’ll be able to keep to that. Construction started in mid-2008, and now, just over three years later, construction is still on track.”
What will follow, in late 2012, is the creation of a much larger, state-of-the-art Emergency Department in the new building, replacing a current ER that was designed to handle much less traffic than it does. Beyond that is deciding what will come of that aforementioned shell space.
But that’s a discussion for down the road. For now, Baystate officials are excited to unveil the results of this ambitious, quarter-billion-dollar investment in the hospital’s — and community’s — future.
Heart of the Matter
As Hunter walked through the new Heart and Vascular space — an ICU floor for more serious patients, two regular inpatient floors, space for outpatient procedures, and a spacious operating suite — he pointed out technology such as the large monitors that loom above the surgical tables.
“Recent technology has improved our ability to do procedures on heart and vascular patients, and that includes a lot of image-guided surgery, which is being able to see the images on the screens as physicians are doing the surgery itself,” he explained.
Most people, however, will first notice the patient rooms, all of them single-occupancy.
“Our current rooms are all double-occupancy,” Hunter said. “But studies show that single-occupancy rooms create an environment for better care and promote patient healing, so that’s going to be one large advantage for patients.
“There are also a lot more opportunities for family interaction with patients, family involvement in care, and making that transfer of care from the doctor and the clinical team to the family, so that when they leave they’re able to have a lot more insight into the care of the patient. There’s also a family area in each room, and family members will be able to stay overnight.”
The hospital is also installing the latest in telemetry and monitoring equipment, as well as the advanced electronic systems already in use to streamline drug prescribing and reduce medication errors.
Outside those hallways, Hunter said, “another thing we’re doing is remodeling the entry to the hospital. It’s sized and configured in a way that, when people come into the hospital, it’s a much clearer entry,” one that funnels patients from a central information desk to either the Daly building or the new structure. Parking has also been reconfigured, with much of Baystate’s north-side employee parking moved off-site to make room for more spaces for patients and visitors.
The second phase of the Hospital of the Future expansion, set to open in the fall of 2012, is a new Emergency Department.
“That was really a response to what our senior leadership heard from the community, from donors, and from staff — that the Emergency Department was greatly in need of upgrading,” Hunter said.
“We’ve been working with clinicians to design a contemporary space that meets the needs of patients,” he continued, adding that the hospital is also working to upgrade the technology and telecommunications systems used in that space.
“The Emergency Department will be three times bigger than it is now, with a dedicated children’s area and new trauma rooms where the most severe patients will be handled right away,” he explained. “The current Emergency Department was built in the ’80s for a much lower patient volume than what they’re experiencing now, so this will be built to the current patient volume.”
Baystate is still trying to determine what to do with space in the current hospital that will be vacated when the Heart and Vascular Program, ER, and other services move to the new building. In addition, the Porter building, which had been used most recently for administrative offices, was torn down to make room for the Hospital of the Future expansion, which looms over Chestnut Street.
Lean and Green
The new building is modern in more ways than one. In addition to how it meets the needs of patients, Baystate engineered several ‘green’ touches. Skylights will bring plenty of natural daylight to interior spaces, reducing energy requirements.
In addition, energy-efficient lighting will be used. Sensors will rely on daylight wherever possible, and lower lighting levels at night. Patient rooms and family areas will be located along exterior walls to maximize access to natural light.
Meanwhile, high-quality window systems will assist with insulation, and the building’s cooling and air-handling systems will be energy-efficient. Baystate has also scheduled large tree plantings along the main road and is constructing a green roof accessible at the third floor but visible from dozens of rooms on higher floors as well.
“It’s an outdoor space between the buildings with a walking trail and benches so that patients, family members, and staff can get outside and get refreshed,” Hunter said. “It’s an amenity to be able to get out there in the sun on nice days.”
Even for those rooms that only overlook the area, “it’s an attractive feature to look out on instead of having a black rubber roof,” he noted. “And there are also environmental aspects; it helps us with temperature control and water conservation, because we collect the water for irrigation.”
Hunter said the project has injected some green of another kind into the area’s construction industry, with between 250 and 300 workers on site daily — about 70% of them based in Springfield or the Pioneer Valley.
“We’ve been able to keep these jobs local because, especially in these times, we know there’s an interest in keeping work local in such an important project for the area.”
That work will eventually slow down, however, and a brand-new building will begin to fill with furniture, equipment, and hospital staff — and the future of Baystate Medical Center will begin in earnest.
Joseph Bednar can be reached at [email protected]

Understanding the Pros and Cons of This Handy Estate-planning Tool
Todd C. Ratner
One particularly useful and common document for this is called a deed with life estate. It has many advantages; however, there are some issues that must be discussed and resolved prior to the transfer to ensure that it will be in the best interests of all those involved.
Demystifying the Deed
A deed with a reserved life estate is used when you wish to both pass your real property to someone upon your death and also protect the property from nursing-home liens. This document may also make it possible for you to live in and maintain control of the property until your death.
The individual or individuals reserving the life estate are referred to as life tenants. The individual or individuals that receive a future interest in the property are referred to as remaindermen. The procedure to complete this transaction involves the execution of a deed, which is recorded in the appropriate Registry of Deeds.
The life tenant has certain duties and obligations to fulfill, including responsibility for paying real-estate taxes and homeowner’s insurance, and making all repairs and performing all maintenance required to keep the property in good working order.
Potential Benefits
There are significant potential benefits when utilizing a deed with life estate.
• Probate avoidance: Upon the death of the life tenant, the life estate is extinguished. The remaindermen become the full owner(s) of the property, thereby avoiding probate. Avoiding probate saves the estate the expense, time, and publicity of the probate process.
• Protection from nursing home liens: A deed reserving a life estate is a gift that triggers a five-year waiting period for Medicaid benefits. Five years after the transfer, the penalty period expires, and Medicaid benefits can be obtained without having to sell the home. Therefore, this technique is best-utilized when it is unlikely that you would be admitted to a nursing home within five years.
• Stepped-up basis: Since your home remains an asset in your estate for estate-tax purposes, at the time of your death, the remaindermen will receive a ‘stepped-up’ basis in the real estate that is equal to the fair market value of the real estate at the time of your death. This means that, when the remaindermen sell the property, they should be able to avoid capital-gains tax if the property does not appreciate in value prior to the sale. This typically helps reduce or eliminate your heirs’ potential tax liability.
Inherent Risks
As attractive as this transaction sounds, there are some potential pitfalls and risks that you should carefully consider prior to executing a deed with life estate. When you sign this document, you give an actual interest in your property to the remaindermen. From that point onward, should you ever wish to sell or mortgage the property, you and all of the remaindermen must agree to do so, and all of you would need to sign the necessary documents.
In addition, in the event that any of the remaindermen experience financial or legal difficulties, such as divorce or bankruptcy, their interest in your property will be considered an asset in the proceedings. As such, you should assess the risk for these potential difficulties prior to transferring your property.
A deed reserving a life estate is not an option to be undertaken without serious consideration. There are other options available when it comes to protecting your home from nursing-home costs or avoiding probate. When determining your best course of action, it is highly recommended that you consult an experienced estate-planning or elder-law attorney so that you understand all considerations, options, and alternatives.
Todd C. Ratner is an estate-planning, business, and real-estate attorney with the law firm Bacon Wilson, P.C. He is a member of the National Academy of Elder Law Attorneys and the Estate Planning Council of Hampden County. He is also a recipient of Boston Magazine’s Super Lawyers Rising Stars distinction from 2007 to 2010; (413) 781-0560; baconwilson.com/attorneys/ratner_2

How to Ease a Loved One’s Transition to the World of Assisted Living

Patrick Laskey says educating families about what assisted living is — and isn’t — goes a long way toward relieving anxiety.
It’s something no one wants to think about, but should.
“In today’s society, seniors are very willing to talk about what they’re going to do early in retirement, and willing to talk about what they’ll do with their estate after they’re gone, but they’re very reluctant to have a conversation about when they will need care,” said Elena Leon, director of community relations for Orchard Valley at Wilbraham.
“They don’t know what needing care means: is it when they can no longer prepare meals? When they can’t walk so well, hear so well, see so well? When it’s no longer safe to walk out of the tub or shower?”
The fast-growing field of assisted living provides an opportunity for older Americans to enjoy the comforts of a home-like setting, plenty of activities and socialization, along with the help they might need — from bathing and dressing to housecleaning and medication reminders — to get through each day.
Yet, many are so attached to the house they might have called home for decades that leaving it is terrifying, even when diminished faculties, and perhaps the loss of the ability to drive, have left them isolated.
“If you’re sitting looking at the four walls or the TV all day, but your human interactions are lost, you may be staying at home, but what’s the value of that life?” Leon asked. “Are you living life, or just waiting for the end? The thing about assisted-living communities is, there’s a life to be lived, so let’s live it, not just look at the calendar and check off another day.”
Administrators at several area senior-care facilities had similar perspectives on the value of assisted living. But the transition from independent living to a different model can still cause plenty of anxiety for seniors terrified of giving up the familiarity of what they have, and families worried about an aging parent’s safety but confused about the care options available.
Patrick Laskey, administrator of Loomis Village in South Hadley, said the challenges of entering assisted living can vary greatly depending on the circumstances surrounding the transition.
“Some people come in crisis; they’ve been alone and independent, or with their spouse, and then some event happens that brings them to the hospital — some difficulty comes to light — and they suddenly need assisted living,” Laskey said. “That’s often the most difficult for residents and families because they’re the least prepared for it. They’re discharged from the hospital, and it’s, ‘oh my God, what are we going to do?’
“They’re under duress, because they haven’t planned it out,” he added, noting that it’s a good idea for families to begin thinking about such contingencies in advance, in case a loved one suddenly does need additional care.
Leon agreed. “I’m a big advocate of having a plan,” she told BusinessWest. “Otherwise, you’re waiting for a hip fracture, or a wandering incident with dementia, or some other precipitating incident that forces the move, and why put yourself and your loved one through that suffering? The last thing you want is to have this suddenly thrust upon you at the hospital bedside.”
In this issue, the BusinessWest explores the questions families must grapple with when a loved one needs more care than they can get at home — and why they shouldn’t put those questions off.
When a House Isn’t a Home

Mary Phaneuf says a house can become a prison for many seniors, and assisted living frees them to keep on living in a quality way.
“They say, ‘I want to keep that house,’ but when the house doesn’t benefit you anymore, it becomes a prison,” she said. “Assisted living opens up opportunities to keep on living in a quality way.”
What is changing is the public awareness of assisted living, a care model between independent senior housing and nursing homes that has come into prominence in the past 20 years, and will continue to grow as the Baby Boomers head into the retirement years.
“Adult children want to see their parents enjoying things, and they see they’ve lost that in their homes — their eyesight is bad, their hearing is bad, they can’t drive anymore, and when they’re home, they tend to isolate themselves,” Phaneuf said. “But when those opportunities are available to them again, they tend to blossom and enjoy life again.
“We don’t cure diseases, and we don’t prevent people from aging,” she added. “We don’t fix any of those things. But we can allow them to enjoy life to the best of their ability until they’re no longer with us. That’s what our goal is.”
But potential residents and families need to educate themselves first on the benefits of assisted living — and to do it well in advance of actually needing it, said Beth Vettori, administrator of Rockridge Retirement Home in Northampton.
“There’s a trend in society that people generally don’t start thinking about whether they need to move or need services until something happens that forces their hand,” she said. “So one thing assisted-living communities do to help facilitate the transition is to offer a lot of programs and informational sessions for families and potential residents.”
Education has become even more important in recent years, Laskey noted, considering that the trend — perhaps driven by economic strains — seems to be people waiting longer to make the move.
“They feel a need to stay in their houses as long as possible, and they’re presenting themselves with a greater number of challenges, in terms of their own health and support,” he explained. “They may have two, three, four chronic medical conditions, and they’re coming in with what we call a higher acuity level, needing more support than in the past.”
Laskey pointed out that educating families about what assisted living is — and isn’t — helps ease anxieties simply by painting an accurate picture of what to expect. And it’s an important part of the process, since the term ‘assisted living’ has been used in the elder-care community to describe a wide range of models, from home care to skilled nursing care.
For Loomis, “assisted living is residential care; it’s a residential environment, not a health care facility,” he noted. “There’s still a lot of misinformation — some people expect a health care facility, and even people who say ‘I want to be independent’ often have a desire for more medical support.
“So we do a lot of educating,” he continued. “Our approach to assisted living is to assist people with being more independent, not to take care of people. We want you to have the highest level of function, comfort, and safety, but people are still independent, and have rights of privacy, self-determination, and choosing their own providers. That’s our day-to-day philosophy here.”
Jacqueline Marcell, an author, speaker, and advocate for elder care issues, also argues for starting the conversation early — while the potential resident is still in good health — in an essay published at www.seniorhousingnet.com.
“Getting them used to the idea beforehand will make it easier when the time comes,” she writes, adding that the senior’s safety is the most important factor, so families should not be deterred by his or her reluctance to discuss the issue.
“If you know that they cannot remain in their home safely, don’t let your emotions override what you know needs to be done,” Marcell adds. “Don’t wait for a broken hip, a car accident, or a crisis call before you step in. Recognize that, when you were a child, your parents would have done everything possible to keep you safe. Now, as hard as it is, you have to be the ‘parent,’ and you have to make the best decisions for their safety.”
Moving Right Along
Even for someone who recognizes the need for assisted living, the move itself can be traumatic, Laskey said, especially if leaving behind a large house, as opposed to an independent-living apartment.
“A major barrier can be how they’re going to downsize,” he told BusinessWest. “That can intimidate a lot of people into avoiding the decision to move — they just have too much stuff.”
To that end, Loomis provides professional organizers to help wade through the downsizing process, which can be daunting, especially for someone who has lived in the same house for many years.
“You can’t fit a 13-room house into a two-room apartment, so you bring the most important things with you,” Leon said, adding that family members can be great helps in whittling down the pile to the most treasured possessions. “You don’t leave your life behind — you take it with you, and look forward.”
She admits it’s not an easy task for many Baby Boomers.
“I’ve moved a dozen times in my adult life, and the next generation [to retire] will probably know how to move, but this current generation, they didn’t move. They didn’t change careers; they purchased or built one home, and that’s still the home they’re in, and they don’t relate to the whole process of relocation. And they can become frozen with fear because it’s too large a concept to think about, and it’s easier to do nothing.”
Vettori stressed the importance of furnishing a unit with the resident’s favorite furniture and decorative items, but just as important is relieving their loved one as much as possible of the burden of the actual, physical move.
“I highly suggest making sure they set up the apartment, cottage, or suite beforehand, so when they person moves in, they’re not faced with that overwhelming sense of, ‘oh my goodness, look at all this stuff boxed up that I have to unpack.’ Instead, they have the ability to walk into a very familiar, very welcoming place.”
Even after the move, many seniors initially struggle with anxiety over this new life, but most adjust well, Vettori said, adding that residents tend to support newcomers with a welcoming committee or buddy system to get them active in their new community.
Laskey said a hospitality committee at Loomis takes new residents under its wing for the first week or so, taking them to dinner and events and basically making the transition as painless as possible.
“We’re not into bringing in people who don’t want to be here and don’t belong here,” he said. “But it can be traumatic when a person moves in; they can feel a loss of individuality, and some have trouble adjusting. That’s not abnormal. But most people stay, and, if you talk to them, most of them love it.”
Leon reported similar experiences at Orchard Valley.
Assisted living is “about safety and care, but also about that social element,” she told BusinessWest. “Aging is not kind, but we want to make it the best, most joy-ridden experience we can. We have to learn how to play again and take pleasure, and not just endure.”
Joseph Bednar can be reached at [email protected]

Recent Study Touts the Value of CT Screening for Lung Cancer

Dr. James Stewart says the CT study is encouraging, but the high incidence of false positives will stir debate over costs versus benefits.
“If I could pick one thing to reduce the cancer burden in this country, it would be eliminating tobacco,” said Dr. James Stewart, chief of Hematology/Oncology at the Baystate Regional Cancer Program. Not only does smoking account for the vast majority of lung-cancer cases, he explained, it’s also a factor in many other cancers, such as stomach, esophageal, and bladder.
Meanwhile, lung cancer is the deadliest cancer in the U.S., with a five-year mortality rate of 10% after the disease has metastasized. The odds of survival are much higher when the cancer is caught early, but right now just 16% of lung-cancer cases are detected in their earliest stages; by the time symptoms typically become evident, the cancer tends to be too advanced to cure.
But a promising study, conducted at UCLA and reported in the June 29 issue of the New England Journal of Medicine, has the oncology world buzzing about bringing that death rate down through widespread CT (computed tomography) screening of smokers and former smokers.
The National Lung Screening Trial (NLST), conducted from 1993 through 2005, involved more than 53,000 people at 33 different sites — all of them at risk for lung cancer but not showing symptoms. The study found that low-dose CT screening reduces the lung-cancer mortality rate in smokers and ex-smokers by 20% due to early detection of cancerous tissue. Many doctors are calling the study a game changer.
“Lung cancer is a very big problem in terms of the number of deaths that it causes,” Stewart said. “It affects both men and women — in fact, a surprising number of women. When I was a medical student, it was rare to see women who had lung cancer; now, there are as many women as men. Men in this country actually slowed down their smoking, and women still have an increasing risk of lung cancer.
“There’s always been this discussion — if we screen people, can we find the lung cancer at a time when it’s curable?” he added. “Because, unfortunately, most lung cancers show up at a time when it’s not curable, when it has already spread, even microscopically.”
A technology proven to catch significant numbers of cancers during treatable stages has, obviously, stirred hope for people with a history of tobacco use.
“There is a population of people who did not smoke but have lung cancer,” said Dr. Neil Chuang, director of thoracic surgery at Mercy Medical Center. “Their cancer may behave a little differently than the one smokers get, but it’s not that common. Smokers would be the ones targeted” by any new national screening protocol.
But the medical community is far from establishing such guidelines, considering the potential financial expense of expanded screening, especially given the propensity for false positives, which — as it has recently with mammograms — will spark a debate over cost versus benefits. But the benefits look promising indeed.
Raising Hope
The response from cancer centers nationwide to the CT report has been overwhelmingly positive.
“I believe that this is not only the best study done on lung cancer mortality, but one of the best studies on cancer screening ever done,” Dr. Otis Brawley, chief medical officer for the American Cancer Society, told CNN.
“With a greater than 20% reduction in lung-cancer mortality, there are very few single things in our lifetime that will have such a positive impact with lung cancer as these new screening suggestions,” Dr. Frank Detterbeck, surgical director of the Yale Thoracic Oncology program, noted on the practice’s Web site.
However, he added, “the NLST addresses a very specific population of people. It will be important to continue to monitor the data and evolve our screening and treatment practices in the coming years so that we can maximize the positive impact it will have on lung-cancer survival rates.”
Chuang said screening guidelines, when they do emerge, might first focus on the heaviest smokers. Currently, between 80% and 90% of all lung cancer is found in people with a history of tobacco use.
“Smokers have an increased risk of having lung cancer,” he explained. “In order to get cancer, a cell has to undergo a series of mutations — usually three or four before a cell becomes a cancer cell. Smoking accelerates that process. The question is, how much smoking is required before the risk goes up?”
He said doctors have settled on 20 ‘pack years’ as the point where the cancer risk rises for smokers. To calculate pack years, multiply packs smoked per day by years smoked; two packs a day for 10 years, or one pack a day for 20 years, would be 20 pack years.
“Most people, when they represent with the symptoms of cancer, are already advanced and not curable,” Chuang noted. “Usually lung cancer is caught by accident, but screening programs are a way of catching it earlier, before it progresses. Right now there’s no standardized policy that I’m aware of put out by any national medical societies, but we’re going in that direction in the next few years, probably for people age 50, 55, or older who have a history of greater than 20 pack years.”
One drawback to widespread screening, Stewart said, is the high rate of false positives when it comes to lung cancer screening. “If you do a lot of CT scans on people who are chronic smokers or former smokers, you’ll find a lot of lung nodules,” he explained.
“The majority of them, by far, are not going to be cancer,” he continued. “So, do you biopsy them with needles? Operate to take the nodules out? Follow up with another CT scan? How do you sort out whether it’s cancer? That’s where the cost comes in, and I haven’t seen a good number crunching of that so far.”
And that introduces the sticky factor of cost also into the picture. While an X-ray is about $50, CT scans typically cost hundreds of dollars. But, according to Brawley, chief medical officer for the American Cancer Society, the average cost of an abnormal spiral CT is about $40,000 to $50,000 once additional testing and possibly surgery is factored in.
“Are you going to implement this as a public health policy, and if so, can you afford it as a society?” Stewart said. “I think those questions have not yet been answered. There are a lot of things we can do using technology that might alter the natural history of a disease in a good way, but it’s not really a question of whether you implement these things; it’s a societal question of where we want to put our resources.”
That debate, he noted, may be influenced by a perception among some people — a kind of discrimination, really — that lung-cancer victims caused their own disease, so therefore society shouldn’t be forced to pour too much of its financial resources into helping them.
“It’s particularly painful for people who have stopped smoking,” he said. “Of course there’s a much higher risk in people who continue to smoke versus former smokers, but there’s no question that former smokers have an increased risk of cancer as opposed to those who never smoked.”
Still, Stewart said, “that conversation is just starting. We’ll see in the next six months or so, some of the major cancer organizations come out with some statements about this. These conversations come at a time when everyone wants to reduce health care costs, or at least slow the increase in health care costs. But it’s still a big story, the idea that screening certain populations of people for lung cancer can be successful.”
Tobacco Road
The CT study isn’t the only exciting news in the realm of lung cancer, Stewart added.
“We’re smarter about lung cancer; it’s not just one disease, but it’s many different diseases, just like breast cancer and colon cancer,” he said. “And the testing of the molecular subtypes of cancer is leading to opportunities to use very specific treatments that will only work in that one subtype. Pathologists are moving fast on this, giving us more information about which lung cancer will respond to which treatment. That’s pretty exciting stuff.”
Still, doctors say, the best way to reduce the risk of lung cancer is simply not to smoke, or at least to quit as soon as possible.
“I always say right up front, if you really want to address lung cancer, you have to address smoking,” Stewart said. “Why we haven’t done a better job of that — well, there are many reasons, but that’s fundamental. Tobacco kills.”
But even quitters — while they’re admittedly at lesser risk than active tobacco users — are far from out of the woods, which is why the recent CT study focused on both smokers and former smokers.
“It’s a lifelong risk, even though you’ve quit,” Chuang said. “A lot of patients I see quit 10, 20 years ago, and they come in and say, ‘I quit; how come I have lung cancer?’ The reason is, by smoking, they may have already caused some of the mutations that cause cancer, and it was only a matter of time before the cell mutations required to transform into cancer cells happened.”
Detecting that progression in time to save lives has long been a struggle for doctors. Now, at least, CT screening can be a powerful tool to help them do just that. Deciding exactly how to wield that tool could prove to be just as challenging.
Joseph Bednar can be reached at [email protected]

Using Photos and Music to Trigger Memories

Steve Berube turned a painful, challenging time in his life into a business that helps people recover their memories.
As a teenager growing up in the music-rich mid-’70s, Steve Berube remembers becoming almost obsessed with the work of Bruce Springsteen.
“I remember being in high school in 1975 when Born to Run came out…” he said, not finishing that thought, but instead shaking his head a number of times to effectively get his point across about how deeply the music impacted him.
He couldn’t possibly have imagined then that, more than 20 years later, subsequent songs from the Boss would help trigger memories of moments he, his wife, Lisa, and their two older children shared together — recollections he thought were lost forever after a horrific car accident in 1995 led to a double concussion, several other injuries, and tormenting memory loss.
Recalling the years after that mishap and his lengthy and difficult recovery, Berube said he would grow increasingly depressed as his daughter and son would play in the room in front of him and he would have to ask them their names. Equally maddening was staring at the seemingly endless array of Disney memorabilia in the Berube home, collected during multiple trips to Orlando, and not being able to remember anything from those excursions.
But then, through a combination of fate, hope, and something approaching science, Berube put together a chronological sequence of pictures of his children when they were young, including several from those Disney trips, and set them, digitally, to Springsteen music — specifically “Candy’s Room” and “The River.”
And some of those presumably lost memories came back.
“I was able to find the path to Disney for a number of things,” he said. “I had recollections of things I couldn’t remember before.”
It would be several years later before Berube would determine that this effective blend of sequential pictures of specific subjects and music to which an individual has an emotional attachment might constitute a successful therapy for some individuals suffering from memory loss.
On that occasion, he created a video featuring a similar mix of music and pictures for a woman suffering from Alzheimer’s, and, more specifically, the occasion of her entering an assisted-living facility.
“Three weeks later, I saw the woman’s daughter at the supermarket,” Berube recalled. “She dropped her bags, ran over to me, gave me a hug, and started bawling; she said her mother had called her by name for the first time in three months.”
Fast-forwarding a little (many more details later), Berube is working diligently toward building a business venture out of what can truly be called his discovery, this blend of two already-recognized memory-loss therapies — music and pictures. It’s called Moving Pictures Inc., featuring a product called ‘photographic journeys,’ or what he terms “cognitive memory therapy for the 21st century.”
The marketing materials recently developed for the product, a clinically based digital video production, says it “walks through a lifetime in pictures and music.” In doing so, that brochure continues, the journey “aims to improve face and name recognition, enhance self-identity, and reduce stress for the entire family.”
The literature makes heavy use of phrases like ‘aims to’ and ‘strives to,’ and the word ‘can’ (rather than ‘will’), because, in reality, the method has been used with only a handful of individuals, but with a high degree of success, said Berube. He noted that ongoing clinical trials involve several dozen people and, he predicts, add several layers of statistical evidence that this process can be a solution for some of those suffering memory loss due to Alzheimer’s, dementia, and head injuries.
Indeed, while developing his product, Berube has studied the suspected link between music and memories extensively, and said his development supports the findings of Petr Janata, an associate professor of Psychology at the University of California Davis and its Center for Mind and Body. Recently, Janata has done extensive work on the relationship between music, emotion, and memory, studying what he calls “music-evoked autobiographical memories.”
“What seems to happen is that a piece of familiar music serves as a soundtrack for a mental movie that starts playing in your head,” he said in a press release detailing his work. “It calls back memories of a particular person or place, and you might all of a sudden see that person’s face in your mind’s eye; we can see the association between those two things — the music and the memories.”
For this issue, BusinessWest takes an indepth look at the concept Berube has developed, as well as the business he’s looking to build from it.
A Discovery of Note
Berube says that, 16 years after the auto accident, he still has issues with short- and long-term memory. Unfortunately, though, one thing he remembers clearly is that early-morning mishap that changed his life in so many ways.
Brought to the surface by hypnosis for one of the legal proceedings that ensued, he said the memories have stayed with him. He remembers that he was heading home from MassMutual, where he worked as a systems analyst, at about 1 in the morning. His normal shift had him working until 3 a.m., but with advances in technology, he and others in that role were able to do more of their work from home, and on this morning he was intent on doing so.
Having made the trek down State Street at that time of day countless times before, Berube said he knew the sequence of traffic lights by heart. As he approached the light at State and Main, it was red, but he knew it would be green by the time he reached the intersection. As he coasted through, however, the car coming south on Main went through a red light, he said, and hit him broadside, propelling his vehicle into the large office building at the corner.
The recovery from numerous injuries was long and difficult, he said, adding that, among other things, he suffered from what he called “unbearable headaches,” which set off deep depression. Later, there were seizures, and tinnitus, or ringing in the ears, has lingered for some time.
There were also the issues with memory and how his brain processed information, which made it impossible to go back to work as a systems analyst, said Berube, adding that, while the inability to resume his promising and fulfilling career was frustrating, moreso was coping — or failing to cope, as the case may be — with the many lost pieces of his personal life.
He was especially frustrated by the fact that he had to keep asking his children their names, even though one of them, his daughter, was essentially named after him; he is Stephen Michael, and she is Stephanie Michelle. “I ended up trying to tie it back that way, and it still didn’t work,” he said.
The memory loss and resulting depression ultimately led him to try various things to bring out recollections.
“I needed to find a way to start being able to look at my kids and know who they were,” he said. “I needed to bring back the memories; I knew we went to Disney — we were Disney freaks and still are to some extent. We had all these pictures and all this stuff, but I had no memories. All these things were a blank.”
And because the house was decorated largely with Disney — his son’s room was “all Lion King” and his daughter’s room was “one of the Disney princesses, I don’t remember which one” — he couldn’t escape the maddening inability to remember.
Eventually, Berube scanned a number of photographs of his children and created what he called “digital videos” of their lives. And when he blended these images with “Candy’s Room” (for his daughter) and “The River” (for his son), some of the memories started coming back.
“I remembered this party we had for our daughter when she was a year and half old. I remember her getting picked up by a Hawaiian dancer. I was able to find that, and when you find things like that, other memories come back.”
Berube told BusinessWest that merely looking at old pictures didn’t trigger such memories. Rather, it was the blending of sequential pictures and music that has meaning in one’s life. Using “Candy’s Room” as an example, he said the song isn’t really about a child’s room, but to him it is, and more than that, it’s a key to unlocking memories of time spent with his daughter.
“That song, and watching that video over and over and over again for hours a day, day after day, week after week, eventually brought things back,” he said, “and it allowed me to start moving forward and not be so depressed about not remembering their names.
“The music, to me, is the key, but it has to be their music,” he said. “It has to be that individual’s favorite music from when they were growing up.”
For the Record
As he talked about how he would eventually take his concept and build a business around it, Berube said that this, too, was a long, trying process. Actually, since the accident, there have a few other forays into entrepreneurship, none of them successful.
One of these was a company that centered around the use of video to help children learn sports activities, such as hitting a baseball or shooting free throws in basketball. It was a good concept, Berube insists, noting that he sunk considerable resources into the venture, but it never took off.
The road to Moving Pictures was paved with the help of a hobby of sorts that he developed — creating videos detailing the lives of the recently deceased. He had created several of these videos, shown continuously at funerals, when he was approached by that aforementioned woman whose mother had Alzheimer’s.
“They got me the pictures, and I sat down at the computer and scanned them in,” he recalled, “and it struck me that her pictures were organized exactly like mine were for my kids. What this woman did was ask her siblings to give her pictures of them and their mom; almost every picture had the mom in it, and each would have a kid and the mom — they were in sequence, with the kid and the mom, until the kid was an adult.
“That brought me right back to my computer in Agawam trying to remember my kids,” he continued. “And I kept the photos in that order. I forget the music I used, but it was great music.”
After that encounter in the supermarket, Berube starting thinking that there was much more to the two incidents than coincidence, and so he continued to do research into the broad subject of memory and, more specifically, the ways in which pictures and music — two therapies that had been tried individually, but not in concert — could help people recover moments from their past.
His research took him to Janata’s work, which seemed to bolster Berube’s contention that music, coupled with carefully arranged pictures, could restore some memories.
“He [Janata] wired people so he could tell which parts of the brain would light up when subjects heard certain things,” Berube explained. “He found that, when people hear songs that they like, a certain part of the brain lights up.”
Other researchers have found that what triggers the memories isn’t the music as much as the emotional attachment to the music, he continued. “As certain songs are played, I can feel myself changing with the song, because each one brings you to parts of your life that your brain is attached to. When you’re young, and you listen to the same song over and over again, like I did with Springsteen, you have emotions tied to that song; that’s what you’re storing. The emotional part is stored forever, so when that song comes up, the part that stores the emotion … lights up.
“We hope that, by lighting up a part of the brain that we know works, we can reteach people,” he continued, adding that, by seeing pictures and hearing music, Berube believes individuals can relearn peoples’ names and remember things from their past.
As he explained how the photographic journeys process works, Berube popped in a display video, the same one that’s on the company’s Web site, www.journeys2remember.com. A composite of random photographs, the video doesn’t represent an actual family, but shows how the process works. Starting with the subject male’s wife, it proceeds to show photographs of an extended family, including children and grandchildren.
Each individual is moved digitally to the center of the photograph, and their name appears on or near the image. There is accompanying information as well, such as ‘first daughter’ and ‘oldest grandchild.’ This chronological collage is then set to music that, in most cases, the individual would have listened to in his or her teens and 20s.
Moving Pictures was incorporated roughly a year ago, and over the course of that time Berube has been hard at work trying to get a business started with what he considers a sound idea, but limited capital. Along the way, five photographic journeys were essentially given away to selected clients, with four of them experiencing positive results — meaning a real difference in their ability to recognize people and recall events — and the fifth at such an advanced stage of Alzheimer’s that improvement should not have been expected, in Berube’s estimation.
After some false starts with the concept, some venture capital has been raised, and an office has been created in Feeding Hills. The plan moving forward is to aggressively market the concept through the Internet and pitches to individual assisted-living communities.
Clinical trials involving perhaps 150 individuals are currently underway, Berube noted, adding that he is confident that the trials will yield considerably more statistical support for the product and act as a strong selling tool.
All the Way Home
Time will tell if photographic journeys can make the leap from clinical concept to successful business product.
Berube knows that, like his road back from his accident and the subsequent physical and neurological ailments, this trek is a long and winding road.
But he firmly believes that the memories summoned by photos of his children and some old Springsteen songs are not the product of chance, but rather a clinical success story he hopes to rewrite for people around the world.
In short, he believes this product, this breakthrough, was — as his favorite musician might say — born to run.
George O’Brien can be reached at [email protected]

Tornadoes Spur New Chapters in Hospitals’ Books on Preparedness

Ann Carroll had already been thinking about tornado preparation when the events of June 1 put Springfield’s hospitals to the test.
This work, which falls under her job description as emergency preparedness coordinator at Mercy Medical Hospital, was inspired by the events in Joplin, Mo. eight days earlier, when a mile-wide tornado devastated that community, killing at least 155 people. It hit the nine-story St. John’s Regional Medical Center head-on, and many of the stories of out of Joplin detailed how the hospital’s staff scrambled to safeguard patients during the few moments of warning they had, and how they carried on, despite great adversity, after disaster struck and cleared the hospital in less than 90 minutes.
Believing there were poignant lessons from Joplin, Carroll started logging information about that event and tornadoes in general to add to Mercy’s database on such matters. What she learned, or had reinforced, among other things, was the fact that tornadoes can ‘hop’ — touching down in one area, rising off the ground for what could be a few hundred yards or several miles, and then touching down again.
“Another thing I learned is that they generally take on the color of the ground,” she said. “If they’re coming just over grass, they’re green, but when they’re black, it means they’re picking up debris.”
Little did Carroll know that, by day’s end, she would have some first-hand knowledge of these phenomena and many others to add to her presentation — which remains a work in progress — and perhaps a few new pages for the binder on the bookshelf behind her desk titled ‘Weather Emergencies.’
Indeed, the series of tornadoes that hit Western Mass. late that afternoon, and especially the one that arrived in downtown Springfield around 4:30, gave new meaning to the phrase ‘learning experience’ for all involved, said Carroll, and in this case provided just one of the myriad ironic twists that fateful day.

Tom Lynch said any emergency plan has a certain amount of flexibility built into it, because it’s impossible to predict precisely what type of disaster will strike.
“One of the things that becomes critical is how you communicate with your staff and how you communicate with the community,” he said, “because, if there’s a need to access services or if there’s a question of whether you should come to work and, if so, how you should do it, then the ability to get that information out becomes a challenge.”
Like Carroll and most everyone else at Baystate and Mercy, he would have some personal accounts to add to his base of knowledge by the time the sun went down on June 1, and some thoughts about where changes or improvement may be needed in disaster readiness. Like Carroll, he said the collapse of cell-phone service was unexpected and problematic. Meanwhile, he said, overall, things could have been much worse that day if, for example, the tornadoes had done considerable damage to one of the arteries it passed right over, including I-91, Route 5, and the Memorial Bridge. And he believes plans should be made for such specific calamities.
For this issue, BusinessWest looks at how Joplin put tornadoes on the radar screen here and elsewhere, in a figurative sense, and how this region’s own experiences brought those lessons home in ways no one could have imagined on May 31.
Getting Wind of It
Recalling the events of that fateful Wednesday, Dan Moen, president and CEO of the Sisters of Providence Health System, which includes Mercy Medical Center, said there wasn’t much talk of tornadoes that morning, and very little in the way of what would be considered heightened alert of additional preparedness other than people “being aware of what could be a pretty significant storm.
“I think that, sometimes, we don’t pay enough attention to those types of storm warnings,” he continued, adding that it’s fair to say that the word ‘tornado’ will never be regarded the same way in this region. “I don’t think anyone will underestimate those storm warnings in the future.”
Although the first tornado touched down in Westfield, and then again in West Springfield, there was very little warning to speak of at Mercy Medical Center, said Carroll, whose basement-level office at Mercy has no windows. She added that there was a warning around 1 p.m. that conditions were ideal for severe thunderstorms and perhaps a tornado, and the first real warning — but for possible tornadoes much further north, in the Amherst/Belchertown area — came at 4:23 p.m., just seven minutes before the funnel cloud then making its way across the Connecticut River showed up on a camera fixed atop the hospital’s roof.
No one at Mercy really knew about the tornado until they heard about that image from the roof camera or saw the funnel for themselves, said Carroll, adding that she was walking through a tunnel between the hospital and Memorial House when the tornado crossed the river into Springfield, and first saw it when she emerged at the other end. She immediately told staffers to seek shelter, and within seconds, warnings had been sent to the pagers and cellphones of employees, and Mercy swung into what’s known as a ‘Medical Alert Code 1,’ the lowest of four levels, with a ‘4’ translating into full-scale evacuation of the hospital.
In the Code 1 scenario, personnel at the hospital were asked to work beyond their traditional shifts (which vary with the position in question), and additional personnel were placed on standby. Meanwhile, patients were moved away from windows — a step already in the response book but reinforced by the events at Joplin — and Moen took up a command post in the hospital’s ER with the mindset that a tornado in an urban area like Springfield could result in a large number of injuries.
“We anticipated that there would be many more victims than what we actually experienced,” he said. “We started to work on the staffing piece — asking people to stay beyond their shifts and calling some people whose skills we knew we’d need, not knowing whether they could get in at that point.”
At Baystate, very much the same thing was happening as that hospital shifted into what it calls a Plan D (for disaster), said Lynch, noting that the facility first went into standby mode for that particular response scenario, and then, when the tornado officially touched down in Springfield, went into the actual Plan D.
There have been a few occasions over the years when this has happened, he said, adding that, in his 16 years at the hospital, the only direct comparison he could draw to the tornado in terms of the type and degree of response and general level of mobilization was the Jahn Foundry explosion in February 1999 that sent 12 workers to Baystate with burn injuries; three of them would later die as a result.
“The similarities are the spontaneity of it, the fact that we had some self-drives — not everyone came by ambulance — and the level of preparation activity,” he said, adding that the nature of the foundry injuries, severe burns requiring that patients be stabilized and then moved to burn centers, made that case different in some respects.
Baystate does not have a specific contingency plan for a tornado, said Lynch, adding that such a development would be covered under what’s known as hazard-vulnerability analysis, which looks at 35 to 40 different things that can happen — from a terrorist attack to a severe blizzard — and prioritizes them in terms of the likelihood of their occurrence, the kinds of damage each might cause in terms of operation, and preparedness level. Tornadoes do not appear on the list (although ‘severe weather’ does), he told HCN, and they’re certainly not a high-priority consideration, or at least they weren’t before June 1.
“When you design a weather-emergency plan, there’s a certain amount of flexibility in there,” he explained. “It might be snow, ice, or severe thunderstorms that take things out of play.”
Imperfect Storm
Given the population density in downtown Springfield and the neighborhoods surrounding it, personnel at both Mercy and Baystate were preparing for a high volume of injuries that, thankfully, never materialized.
At Baystate, for example, the hospital moved into what the system calls ‘mass casualty mode.’
“With the damage you’re hearing about — with the collapses, the closed-off neighborhoods, and the closed-off streets, the anticipation is that you’re going to get large numbers of wounded people here,” Lynch explained. “So you move into the mass-casualty mode, which then ramps up different aspects of the operation, particularly the clinical things.”
Elaborating, he said that Dr. Reginald Alouidor, attending physician in Baystate’s Level One trauma unit, the only facility of its kind in Western Mass., was forming trauma teams, and the Emergency Department staff were moving patients and creating room for a crush that was far less severe than it could have been.
Baystate eventually treated 25 people, 10 of them in the trauma unit; seven were admitted. Mercy, meanwhile, treated a total of 35 people, none of them with life-threatening injuries, and all were treated and released.
Many of these individuals transported themselves to the hospital, which made this situation unique in some ways. “I remember this one car that drove up … the roof was V-shaped,” said Carroll. “A tree had fallen on top of it, and the windows were blown out; there was a baby in the car, and they needed two wheelchairs to get the occupants out and into the emergency room.”
While dealing with the injured from the first tornado, both hospitals soon went on alert for more twisters, especially one that was reportedly moving southwest from Chicopee, right into the path of the two facilities.
Moen said these reports prompted staffers to once again move patients away from windows and consider additional steps to ensure both patient safety and efficient handling of large numbers of injuries.
When asked what lessons Mercy and other hospitals could take away from the events of June 1 — just as they are all learning from Joplin — Carroll started with the need to pay a little more attention to the weather, a need she’s already addressed.
“Someone told me Radio Shack was having a special on hazard-alert radios, for $29.99,” she said. “They were getting rid of last year’s models, so I went and bought five of them; we’re going to place them at the security booth, the front desk, at the switchboard, which is also in the basement, and the fourth floor of the Weldon Center, because they saw it out the window about the same time I did.”
Beyond that, she and Lynch said much of the focus has been on the ineffectiveness of cellphones — again, something that wasn’t anticipated — and steps that may be taken in the future as a result.
“I received only one call in two hours, and every call I tried to make didn’t go through,” she said, adding that backup contingencies, ranging from land lines to two-way radios to texting, kept most of the lines of communication open.
In the wake of the tornadoes, Mercy will look into having more ham radios tuned to the SkyWarn channel, another stormchasers’ outlet. “Many times, they’re the first to see the first touchdown.”
Said Lynch, “It’s a stunning thing for people to dial something on a cell phone and get busy circuits all the time. You have to look at what that impacts. It didn’t affect our operations, but when you live though it like this, you ask questions about what happens next time.”
As is typical with such events and the drills that replicate them, he added, there is a comprehensive debriefing exercise, at which those involved discuss what went well and what didn’t. In this case, most all matters fell into that first category.
“But in this particular case, we’re going well beyond that, because it was an actual event, and we’re really soliciting information from our clinical people,” Lynch said. “They did fabulous work, and they organized this so rapidly; it’s not a surprise, but it’s always great to see. People take the training, and they take the understanding, and they do what they have to do, and do it remarkably well.”
Lasting Impressions
Caroll is still working on that PowerPoint presentation she talked about. The pictures and accounts of the Joplin disaster offer some important lessons for Mercy and all hospitals.
“We wanted to look at the types of damage done to the hospital in Joplin, and the things that we would need to consider in our planning,” she said, “such as the safest places to seek shelter in the buildings, warning systems, and so on.”
All that will still go on, but now there are other, far more personal accounts of what to do when a tornado strikes. They are one of the more positive things to take away from a day that won’t ever be forgotten. n
George O’Brien can be reached at [email protected]
A list of area physician groups and their specialties
Click Here: PhysicianGroupsBW0711a

How Best Buddies Helps Young People Come to an Understanding

Theresa Ruszczyk (right) and her buddy, Lucy Pasche, say their friendship has benefited both of them in several ways.
This synopsis, known in the parlance as a ‘friendship update,’ does a remarkable and efficient (just 139 words) job of explaining just what the program Best Buddies is all about, and how it creates an abundance of those grammatical smiley faces like the one seen at the end of this missive.
Written by a young woman from Northampton, this monthly update report tells of how two people have become, well … buddies, and how they are spending increasing amounts of time together, finding out about one another, supporting each other, and anticipating a relationship that will continue to grow.
Better than any lengthy brochure, this simple update gets to the heart of the matter when it comes to Best Buddies, which pairs individuals who have intellectual and developmental disabilities (IDD) with people of the same age who do not. New friends, or buddy pairs, commit to contacting each other weekly and participating in a one-to-one activity together monthly. In addition, members plan and participate in at least four group activities each year.
Participation in the program becomes a unique growing and learning experience, said Kate Crowther, director, since last fall, of an area that includes Central and Western Massachusetts.
“While there is a service component and a mentoring component to the programs,” she explained, “we really try to support and enforce the idea that each student is of service to the other; it’s a mutually benefiting relationship. And so it’s not about spending an obligated amount of time with someone to fulfill your own personal desire to be of service to someone — it’s about taking steps to become more aware of people with intellectual and developmental disabilities, what their capabilities are, and to integrate the two demographics together.”
Theresa Ruszczyk (pronounced ruzz-ik) would certainly agree.
A junior at Northampton High School, she’s been involved with Best Buddies for two years now and is currently president of the Northampton Club, as these groups are called. At a matching party last fall, she was paired with Lucy Pasche, a senior at NHS who has Down syndrome.
Over the past several months, the two have gone to a number of Best Buddies-organized events together, including a dance, a few movies, a day of ice skating, a Halloween party, and a holiday-season get-together at which participants crafted gingerbread houses to be displayed in downtown businesses. Meanwhile, they ‘talk,’ which usually means texting, every day, and have formed a friendship that has benefited both young women in a number of ways.
“I’ve gained a lot more respect and patience and the knowledge that everyone is capable of doing something,” said Ruszczyk. “I’ve realized a lot more about everyone, especially people with disabilities. I never look at Lucy and think about what she can’t do. I’m focused on what she can do, like run track and be a team captain, be a teacher’s assistant, and much more.”
Meanwhile, Pasche used the phrase “that was fun” to describe a number of the activities that have been part of the Best Buddies experience, especially the dance and gingerbread-house-building activities.
For this issue, BusinessWest takes an indepth look at Best Buddies and how Crowther is being aggressive in her efforts to build awareness of the program and thus create more opportunities for those smiley faces and strong relationships like the one forged by Theresa and Lucy.
The Buddy System
When asked about these efforts to raise the profile of Best Buddies in her large region, Crowther offered a significant sigh and a telling smile.
“It’s a 24/7 effort,” she said, adding quickly that she was exaggerating, but only slightly. Indeed, getting the word about this organization and expanding its already considerable footprint constitutes the top line of Crowther’s job description. It’s an intriguing challenge for an organization that locally is far less a household name than its leading spokesperson — New England Patriots quarterback Tom Brady.
But it has made significant strides over the past several years, said Crowther, noting that the area she leads now boasts more than 800 members and 19 chapters involving colleges, high schools, and a few middle schools.
In Western Mass., the colleges are Mount Holyoke, Smith, Springfield, and UMass Amherst. Meanwhile, there are eight area high schools involved — Amherst, Athol, Chicopee, Minnechaug, Monument Mountain, Northampton, Pittsfield, and Westfield — and two middle schools, Amherst and Glenbrook, both in Longmeadow.
Crowther said her twin goals are to grow the number of chapters — to the extent the budget will allow — and strengthen existing programs. This is what’s happening nationally and internationally for an organization started in 1989 by Anthony Kennedy Shriver and that exists with the ultimate goal of essentially putting itself out of business.
“We enhance the quality of life for people with IDD,” Crowther explained, “while striving toward our long-term goal of establishing a society in which people with IDD are so successfully integrated that our services are no longer needed.”
Best Buddies pairs non-disabled students (peer buddies) with individuals (participant buddies) who have intellectual and developmental disabilities such as Down syndrome, autism, William’s syndrome (a genetic condition characterized by medical problems, including cardiovascular disease, developmental delays, and learning disabilities), Asperger’s syndrome, and other conditions.
The Boston-area office of the organization opened in 1995, said Crowther, and as demand for such programs in the central and western parts of the state grew, an office to serve that large region opened in 2005. It operates with the same guiding principles as the others, and that overriding goal of creating learning experiences for all those involved.
The many benefits of the program can be seen in the findings of a study conducted at Yale University in 2005. “Best Buddy relationships appear to offer unique benefits to the psychological adjustment of adolescents with mental retardation,” wrote the physicians who conducted the study. “The frequency of contact [adolesecents with intellectual disabilities had with their non-disabled peer buddies] was associated with lower frequencies of peer victimization, better adaptive behavior, higher levels of self-esteem, fewer psychological symptoms, and increased socialization.”
Equal Share
They can also summarized in an annual survey of the Best Buddies program conducted by Michael Hardman, dean of the Department of Special Education at the University of Utah. Results of several recent years showed that:
• 90% of high school peer buddies and 86% of college peer buddies have a more positive attitude about people with intellectual disabilities;
• 80% of the participants with intellectual disabilities demonstrated improved social behaviors;
• 77% of special-education faculty felt Best Buddies heightened awareness of the special-education department and its students among other faculty and non-disabled peers;
• 74% of the participants without intellectual disabilities were more aware that people with intellectual disabilities can hold jobs; and
• 92% of high-school peer buddies (without intellectual disabilities) and 85% of buddies with intellectual disabilities viewed their Best Buddies experience as enjoyable. Meanwhile, 97% of college peer buddies and 83% of college buddies viewed their Best Buddies experience as enjoyable.
“As with any successful social movement, the key to reform is changing people’s minds and hearts,” Hardmann wrote. “By introducing one person with a disability to a peer who does not have a disability, Best Buddies Massachusetts meets the immediate need for socialization and effects long-term change in people’s attitudes toward those with intellectual disabilities.”
Ruszczyk said the Northampton chapter has grown and evolved over the past few years. When she joined, most members were seniors, and when she graduated, the chapter had just a handful of participants. But it has grown to nearly 50 over the past year.
Some of these members have buddies, but many do not (lack of transportation often makes it difficult to meet some of the requirements), and these individuals are essentially friends to all those with IDD, said Ruszczyk.
“They don’t look at not having a buddy as being a barrier,” she explained. “They went beyond that; they’re very social and friends with everyone.”
“We want to be as welcoming as we can,” she continued, adding that the chapter’s get-togethers are open to all students at the school, not simply members. Meanwhile, the Northampton chapter will collaborate with the one at Amherst High School on events to create larger gatherings that help build awareness of the organization and its many goals.
By building greater awareness, Crowther hopes to be able to take the Best Buddies model to more middle schools, high schools, and colleges in Western and Central Mass., and, ultimately, make her region self-sustaining.
Achieving this goal will require greater financial stability and flexibility, she continued, adding that Best Buddies Massachusetts provides most of the funding for the regional office, but grants have also been secured and several fund-raising events have been added in recent years to provide that stability.
A fashion show staged at Thornes Market in Northampton this past spring was one such activity, while a golf tournament, slated for later this month, is another. The most successful fund-raiser to date, however, is an endeavor known as Artistic Abilities, an event that showcases and various talents of area buddies. Artists from the community will partner with individuals involved with Riverside Arts Industries, an Easthampton-based organization that provides services to those with intellectual and developmental disabilities.
Moving forward, the organization wants to take its fund-raising activities to a higher level, she continued, but from a big-picture perspective, the success of best Buddies lies in relationship-building on a number of levels — with participating schools, area businesses, and the community at large.
Getting Together
Pasche will be attending Holyoke Community College this fall, with a specific course of study to be determined later. Ruszczyk, meanwhile, is just starting the process of looking at schools, and for now, she’s equally undecided about a career path.
One thing she has decided is that she wants to continue her involvement with Best Buddies. “I hope the school I go to has a chapter — I’m pretty passionate about it,” she told BusinessWest, to which Crowther replied that, if that institution didn’t, she could always try to start one.
But that’s down the road. For now, she and Pasche are focused on the summer, finding ways to stay in touch (a cell phone greatly facilitates that process), and building upon a friendship that has already provided some enduring memories and important lessons that will linger well beyond their time at Northampton High School.
And that, in a nutshell, is what Best Buddies is all about.
George O’Brien can be reached at [email protected]
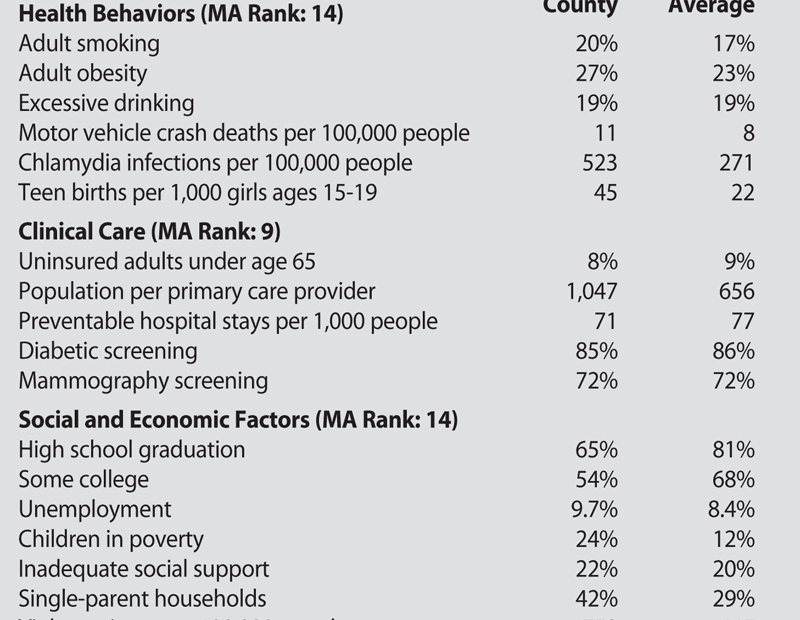
The Roots of Hampden County’s Health Problems Run Deep

Dr. Andrew Balder says the socioeconomic data behind Hampden County’s health ranking is impossible to ignore.
Is Hampden County the least-healthy county in Massachusetts?
Well, the numbers don’t lie, but they also point to factors that run well beyond — and much deeper than — access to quality care.
That’s the message conveyed in a recent survey of every U.S. county. The 2011 County Health Rankings — produced for the second straight year by the University of Wisconsin Population Health Institute and the Robert Wood Johnson Foundation — ranks Hampden County 14th among 14 counties in Massachusetts in overall health.
Initially, that might seem like a slap in the face to a region that’s home to many high-quality hospitals and other health care providers, but a closer look reveals issues that can’t be solved by the medical establishment.
“You can always question the data, but there’s reality behind it,” said Dr. Andrew Balder, attending physician at Baystate Mason Square Neighborhood Health Center and medical director of the Boston Medical Center HealthNet Plan.
He noted that socioeconomic factors played heavily into the rankings, putting many urban centers — which tend to be home to significant pockets of poverty — at an immediate disadvantage (Suffolk County, containing Boston, ranked 13th). The survey gave 10% of its weight to a county’s physical environment, 20% to clinical care, 30% to health behaviors, and 40% to social and economic demographics.
“It does take a village,” Balder said. “This is a direct reflection of Hampden County, of the difficulties of a county dominated by one poor city — Springfield — and a second, smaller, poorer city, Holyoke.”
Dr. Franklin Robinson, executive director of Baystate Health’s Partners for a Healthier Community, agreed. “If you look at the urban core on this county — Springfield and Holyoke — those two centers probably account for the majority of the county’s bad report, because these are problems that really concentrate in urban centers,” he said.
“That tells me this county is really healthier than we suspect, but the urban centers are that much more dramatically challenged, and that brings down the entire report,” he added. “It also signals that these are population-level problems that require much more than tinkering.”
The survey ranks Hampden County well below the top duo of Nantucket and Dukes counties, which represent the islands south of Cape Cod, but that’s not a useful comparison, said Dr. Garry Bombardier, medical director of the Work Connection at Holyoke Medical Center.
 “I know everyone wants to compare us to Dukes County, but that’s a very different part of the world,” he said. “It’s more helpful to take a look and compare us to the next county over — Hampshire County, which turned out to be fifth.”
“I know everyone wants to compare us to Dukes County, but that’s a very different part of the world,” he said. “It’s more helpful to take a look and compare us to the next county over — Hampshire County, which turned out to be fifth.”
And some of the comparisons are striking. The premature death figure — which calculates total years of life lost before age 75 — is 44% higher in Hampden County than in its northern neighbor, owing partly, of course, to the much higher rate of violent death in young people endemic to many cities like Springfield.
On the other hand, Bombardier said, “low birth weight in babies is very often an indirect measure of health care, nutrition, and economic status.” On that count, 8.6% of Hampden County babies are born underweight, as opposed to 6.4% in Hampshire County.
He cited other disparities between the two Pioneer Valley counties — a teenage birth rate of 4.5% in Hampden County and 0.7% in Hampshire County; high-school graduation rate, 65% and 85%; unemployment, 9.7% and 6.6%; single-parent households, 42% and 25%; children in poverty, 24% to 10%; and a violent-crime rate three times higher in Hampden County than in Hampshire County, to name a few.
“Again, this is taking a look at the fiber of our society, and it has to do with education, with social and economic factors, do you have jobs, things like that,” Bombardier said. “It’s a very big difference, and we should really be paying attention to it.”
The authors of the study recognize that they’re casting a wide net. “The rankings really show us with solid data that there is a lot more to health than health care,” said Dr. Patrick Remington, the project’s director, when the report was released earlier in the spring. “Where we live, learn, work, and play affect our health.”
Many Miles to Go
The report comes as no surprise to Mark Fulco, vice president for Strategy and Marketing for the Sisters of Providence Health System, who conducts a detailed community-needs assessment as part of the system’s overall planning and resource allocation.
The Wisconsin study “really deals with a lot of those issues,” he explained. “One of the things we look at is a community needs score; we look at each ZIP code and come up with a score from 1 to 5, with 5 representing the highest needs, based on factors like poverty rate, unemployment, and insurance coverage.”
Springfield, Holyoke, and parts of Chicopee all score very high on that scale, Fulco noted, adding that populations in this range are more likely to wind up in the hospital for conditions, like pneumonia and congestive heart failure, that people in communities with better socioeconomic scores are more likely to handle through primary care.
“If poverty influences health to a significant degree, then the [last-place] ranking is appropriate,” Balder said. “It’s part of the underlying environment that creates an unhealthy physical and social environment. It makes individual healthy behaviors more difficult to attain, and when you make the barriers higher and stack the decks, it becomes harder and harder to act on healthy decisions.”
Fulco cited a survey conducted by the Mass. Executive Office of Health and Human Services, which asked residents to rate their own health, and 21% of Springfield residents rated it ‘fair’ or ‘poor’; the state average was just over 12%.
“No wonder the report ends up where it does,” Fulco said, also citing asthma rates, tobacco use, inadequate prenatal care, and other factors in which Hampden County posts numbers nearly double the state average. “The magnitude of the problem is substantial. We’ve got a societal challenge, and it’s important to put public resources toward addressing these needs.”
As a health system, Fulco said SPHS is doing exactly that, from its mental-health programs run through Providence Behavioral Health Hospital to its participation in REACH programs in area schools; from its community health screenings to its Vietnamese Health Project that strives to reduce barriers to health care for the city’s Vietnamese population. “We know we are here to serve our community, and our services need to reflect that,” he said.
Robinson mentioned some community-based projects aimed at reversing some of the underlying factors highlighted in the report.
“The good news is that, in our local communities, there have been some neighborhood groups working together to affect some of these indicators,” he said, citing projects like the Mason Square Health Task Force, the North End Campus Coalition, and others that emphasize economic development alongside social needs.
“We’re beginning to look at the human social issues affecting residents,” he said. “In some of our most challenging neighborhoods, whole collections of people are trying to figure out how we can improve quality of life and the economic experience of our communities and, consequently, the health and well-being of the people who live there.
“It’s a public-health situation; it’s not just a health care problem,” he added. “To change our county’s health status, people need jobs, and they need housing. Essential to good health is the ability of a family to live in an economically self-sufficient manner.”
Some of the long-term statistics have been distressingly consistent, Robinson noted. For instance, infant mortality among African-Americans in the region is about three times that of white infants — the same gap that was present 30 years ago. “That’s a hard indicator that we haven’t been able to effectively organize our resources. We have not made an impact on changing that rate.”
And that’s just one of many stubborn trends, he said. “That’s what makes this so daunting — there isn’t a simple solution out there; there isn’t just one way to do it. How do we, as a community, work to achieve collective impact?”
A Call to Action
Like the others who spoke to BusinessWest, Balder believes the effort is worth it.
“Just because a community is poor doesn’t mean people have to be unhealthy,” he said. “A community can become healthier even though it’s poor. You can throw your hands up and be defeated, or keep working.”
The report’s authors claim that several communities across the U.S. have begun to take action in response to last year’s study, such as passing smoke-free laws, boosting educational opportunities for young children, and pushing for healthier grocery stores and farmer’s markets. But those who work with public-health issues in Hampden County have long been aware of the region’s needs.
“It’s more than the medical delivery system,” Bombardier said. “We’re definitely seeing more people dying younger and more low-birth-weight babies, who require lots more care, and many of them require special education later in life to get them back up to where they belong. We can see the results of poverty, of not having educated people, of not having enough primary-care providers. It’s an overall problem with our community.”
Dr. Risa Lavizzo-Mourey, CEO of the Robert Wood Johnson Foundation, noted that “it’s hard to lead a healthy life if you don’t live in a healthy community.” But the inverse is also true — communities don’t get healthy unless their residents start living healthy lives.
And despite the well-documented barriers, “we have a very bright community with some very active people,” Bombardier said. “My hope is that this will spur people to look at what we can do to make a difference.”
Joseph Bednar can be reached at [email protected]

Misconceptions Persist on Stuttering, Its Causes, and Treatment

Nadia Dorval says using the phone is so difficult for people who stutter that they usually avoid it.
But, although the monarch experienced success, there is no cure for stuttering, and more than 3 million Americans and 68 million people worldwide live with the problem every day. Winston Churchill, Marilyn Monroe, and Carly Simon are a few of the well-known figures who number among their ranks.
“Many famous people were stutterers. It has nothing to do with intelligence. But people who stutter often have a sense of inadequacy and feel frustrated, angry, and depressed,” said Nadia Dorval, an adult speech language pathologist with Baystate Rehabilitation Care in Springfield.
“For some people, stuttering is developmental and can change, and for others it is chronic,” said Karen Spinelli, a speech-language pathologist at Noble Hospital in Westfield. “People usually start to notice it when children are preschoolers or about the time when they begin developing language.”
According to the Stuttering Foundation, the condition affects four times more males than females, and approximately 5% of all children go through a period of stuttering that lasts six months or more. Three-quarters recover by late childhood, and about 1% have long-term problems.
Dorval says stuttering in adults doesn’t always begin in childhood and can be caused by an injury to the brain. “It is not something that’s black and white; stuttering is very complicated,” she said. “People have the misconception that stutterers can control their problem, but even when they do, it can occur again in high-stress situations.”
For this issue, the BusinessWest looks at the causes of stuttering, what adults can do to help children who stutter, and why unrealistic expectations and a fast-paced lifestyle can make the situation worse.
Early Speech

Karen Spinelli says materials from the Stuttering Foundation can help people become informed about the problem.
She explained that three things are necessary for speech: breathing, voicing, and articulation. Voicing refers to the way the muscles of the vocal cords close and vibrate, while articulation is the way the lips and tongue move to produce sound. “Researchers tell us there is no one definitive cause in developmental disfluency,” Spinelli explained.
However, research is beginning to show that there may be a genetic component, and Spinelli says the latest findings reveal a difference in the way the brain controls the three main areas of speech in people who stutter.
Environment also plays a role. “It doesn’t cause stuttering, but can make it better or worse. The more anxious a stutterer becomes, the more it can exacerbate; stress and anxiety can cause a snowball effect,” she continued, adding that staying relaxed while speaking is critical for stutterers.
If a child begins stuttering, all of the adults in his or her life should behave in the same manner, said Spinelli, who advises them to talk slowly in a calm manner, to avoid looking worried or rushing the child, and to pause before they respond to what the child says.
“Don’t jump to answer the child quickly, and maintain eye contact so they don’t feel you are losing interest,” she continued, adding that adults should never try to help a child by finishing their sentences. “It is important for a child to feel they have your attention. If you speak for them, it can send the message that they are inadequate and create more anxiety. It is important for the child to know that what he or she is saying is more important than how it comes out, even though it can be difficult to take the extra time to listen.”
The reason speaking slowly makes a difference is because people tend to match the rate of the speech of those around them. “It is a very unconscious behavior,” Spinelli said.
Another helpful technique is singing or reciting nursery rhymes out loud with the child. “People who stutter don’t usually exhibit the behavior when they are singing or talking in unison, so it’s a good idea for parents to do these things with their child,” she told BusinessWest.
However, if frustration arises, parents should ask their pediatrician to refer them to a speech-language pathologist. There are early-intervention programs for children younger than age 3, and after that, the school department can help. “Most people don’t realize that, even if a child is not in school yet, he or she can still receive services through the school system,” Spinelli said.
Claudia Eitnier, a speech language pathologist at Mercy Medical Center, said one of the reasons it is prudent to seek an evaluation is because the stuttering may be part of a broader speech-and-language problem. “Don’t become impatient when someone stutters, and don’t treat a child or adult who is stuttering as if something is wrong with them,” she said. “It is not something the person is doing intentionally.”
Myths Abound
There are a number of myths related to stuttering. These include the thought that people who stutter are less intelligent, that the condition is caused by nervousness, that it can be ‘caught’ by imitation or hearing another person stutter, that it is caused by stress, and that it helps to tell a person to “take a deep breath before talking,” or “think about what you want to say first.”
None of these things are true. People who stutter can become nervous due to other people’s reactions, and stress can make it more difficult for them to speak fluently. But these things do not cause the problem.
The purpose of therapy is to provide people who stutter with useful strategies and help them learn ‘easy stuttering.’ This refers to teaching a person to speak with less tension in their throat and mouth.
“It makes the stuttering less pronounced,” Spinelli said. “The more emotionally anxious a person becomes, the more tense their muscles become, and the worse the stutter becomes.”
Stuttering does tend to decrease as children grow, she added, but can occur again at any point in their lives. In fact, the goal of stuttering therapy isn’t always to make it go away.
Eitnier says technology can be useful in treating some cases of stuttering. One device used by therapists is called Speech Easy. It resembles a hearing aid, and provides delayed auditory feedback, allowing the person to hear their speech at a different pitch with a slight time delay.
“This causes the person to change their pattern of speech, and usually results in the reduction or elimination of stuttering,” she explained. “Hearing their own words played back changes the mental processes that coordinate speech.”
Biofeedback programs can also be helpful. One program works by having a person speak into a microphone while wearing a headset and listening to music or background noise. The person can see the pattern of their speech on a computer screen, and the background noise, which blocks the sound of their voice, can make speech easier for some people.
“But there isn’t one right way to treat stuttering,” said Eitnier. “Since no two stutterers are alike, what works for one may not work for another, because its roots, causes, and severity vary. And even though there is no cure, pill, or surgery for it, people can learn to manage their stuttering.
“But it is very hard work no matter what age you are,” she continued. “Adults are taught relaxation techniques; the more relaxed and comfortable they are, the more fluent they become.”
Dorval sees many adults who stutter, and says some re-learn strategies taught during their childhood. One is to stop speaking and take a deep breath from their diaphragm when they begin to stutter. “The whole idea is to remain relaxed,” she said. “Stuttering typically happens when they are in an emotional or stressful environment. If they become angry or excited, emotions can take over their speech.”
Speaking on the phone is also difficult, because stutterers fear judgment and often don’t know who will answer when they make a call. “Most stutterers will tell you they hate the phone. They will text people or use e-mail and have other people make their doctor’s appointments for them,” Dorval said.
One technique she uses to overcome this is to have an adult call stores and ask if an item is available. They prepare a list of questions before they call, and then read them off from a checklist. Dorval advises them to take their time, speak slowly, and if they begin stuttering, to stop, take a deep breath and then begin speaking again.
“A lot of stutterers talk very fast; some repeat entire works, some repeat phrases, and some repeat the initial consonant sound. And some also use interjections such as ‘ah’ or ‘um’ between words and have hard or soft blocks,” Dorval said, adding that a block refers to the length of time that passes between words or sounds.
“A soft block may come across as inappropriate pausing while a hard block makes the words sound tense,” she explained.
Recording the person’s voice while they are speaking, then playing it back to them can also be useful. “If they hear what they doing, they can see where they could have slowed down and started again,” Dorval said.
Some stutterers develop secondary behaviors such as rubbing their leg or wincing when they speak, she continued. These actions take place because at some point, the behavior worked and as a result it became an involuntary response.
“I worked with someone who rocked and bit his hand while he spoke, and had someone else who would wring her hands,” she told BusinessWest. “The behaviors create more tension, and part of the person’s therapy is to make them aware of what they are doing, because these actions make their stuttering more obvious.”
Dorval wants adults to know that if they are talking to someone who stutters, they should not finish their sentences or interrupt the individual. “People want to help, but they need to be patient. And if you work in a public place and get a stutterer on the phone, be extra patient. It takes a lot for them to make a call,” she said.
Adults who stutter often report they have difficulty with job interviews and relationships. “They feel like they are not capable of interacting the same way as someone who speaks fluently,” Dorval said. “But if someone really wants to improve, and is ready to make a commitment, the chances of a successful outcome are increased.”
Navigating the Minefield of Long-distance Caregiving

By Gina M. Barry, Esq.
It is also common for an elder to be unwilling to move closer to their family, even if staying where they are means receiving care from someone other than their family members. Although the distance creates many hazards, steps can be taken to allow successful navigation of the minefield of legal, financial, and administrative issues that lie in wait for the long-distance caregiver.
The most common legal issue associated with providing proper care and oversight from a distance involves establishing proper legal authority to ensure ongoing care in the event of incapacity of the elder. When proper legal authority is not established, caregiving can be interrupted, leaving the elder at risk for physical, mental, and/or financial harm.
This legal issue can be easily resolved through the elder’s execution of a durable power of attorney and health care proxy. The durable power of attorney and health care proxy are two distinct legal documents that give a person the elder chooses the authority to make financial and medical decisions on the elder’s behalf if the elder is incapacitated.
In the event that a durable power of attorney and health care proxy are not established and the elder loses capacity, it will be necessary to petition the probate court to appoint a conservator and/or guardian to make financial and medical decisions for the elder. The process of having a conservator or guardian appointed is expensive, time-consuming, and results in the elder’s loss of privacy and legal rights. As such, the overseer of the elder’s care should discuss with the elder the need to establish these documents while the elder is still capable of executing them.
In addition, end-of-life decisions should be discussed with the elder, and the elder’s wishes should be memorialized in writing within the proper legal document. Ideally, the estate plan will also include a will, which provides clear instructions as to the disposition of the elder’s estate upon their passing away.
Because the law varies from state to state, another common legal pitfall arises when the estate planning documents that have been established are not valid or are not recognized. This pitfall usually arises because: (1) the documents were not properly prepared or executed; (2) the documents were prepared in the caregiver’s state and are not recognized in the elder’s state; or (3) the documents were prepared in the elder’s state and the elder moves to the caregiver’s state where documents are not recognized.
To avoid the pitfall of having unusable estate-planning documents, it is best to hire elder-law attorneys practicing in both the elder’s and the caregiver’s states, so that you can be sure the advice you receive will pertain to the law of each state, and any necessary state-specific provisions will be incorporated into the estate-plan documents. Otherwise, it is possible that the elder could lose the protection of the documents, especially if the elder moves after losing his or her capacity to execute new documents.
Financing care is another area loaded with potential problems for the long-distance caregiver. Many times, the elder expects that public benefits (Medicaid) will pay for his or her care needs. Again, each state has different rules relative to obtaining approval for public benefits, and there are vast differences between the states as to various issues, including, but not limited to, asset and income limits, the effects of long-term-care insurance, and the effects of past gifts. Again, it is imperative to consider the rules in both states when planning if there is any possibility that the elder will relocate.
Further, there are also differences in the reach of each state’s estate-recovery rules, which are the rules that allow the state to recover benefits paid for care from the estate of a recipient who has passed away. Here, proper planning can ensure that benefits will be obtained as efficiently as possible and, at the same time, minimize the exposure of the elder’s estate to recovery efforts.
With respect to administrative issues, coordinating caregivers can be a daunting task. It can also be a serious mistake to rely on an elder’s self-reported care needs, because many do not recognize their own needs when they arise. As such, every long-distance caregiver should hire a geriatric care manager in the elder’s area. A geriatric care manager is a health care professional with training in gerontology, social work, and nursing. In most cases, the geriatric care manager will conduct an assessment of the elder and develop an individualized care plan.
In the long-distance-caregiving situation, the geriatric care manager will act as a liaison for the distant caregiver. Here, the geriatric care manager will oversee the elder’s care, providing a report to the caregiver at regular intervals and alerting the caregiver to any potential problems. The geriatric care manager’s additional oversight not only provides peace of mind for the long distance caregiver, but also guards the caregiver from claims that he or she is not conscientiously carrying out his or her duties due to the distance and/or lack of personal oversight.
Even though long-distance caregiving is a minefield, the wisest of caregivers knows that hiring professionals in the elder’s area, the caregiver’s area, or both is the equivalent of employing a minesweeper. With proper planning and the advice of elder-care professionals, caregivers can defuse or altogether avoid the mines and successfully navigate the minefield of long-distance caregiving.
Gina M. Barry is a partner with Bacon Wilson, P.C. She is a member of the National Assoc. of Elder Law Attorneys, the Estate Planning Council, and the Western Massachusetts Elder Care Professionals Assoc. She concentrates her practice in the areas of estate and asset-protection planning, probate administration and litigation, guardianships, conservatorships, and residential real estate; (413) 781-0560; baconwilson.com

In the Trauma Bay, Work Is Carefully Choreographed

Dr. Reginald Alouidor, here consulting with surgical residents, says work in the trauma unit is a total team effort.
It is 4:56 p.m., and Dr. Reginald Alouidor is looking at his pager.
It is alerting him to the fact that an elderly woman is being transported from Cooley Dickinson Hospital in Northampton to the trauma unit at Baystate Medical Center. She had fallen in her home, suffering injuries to her face, as well as a broken wrist, but there are fears that she has also sustained brain injuries. “She was stable, but there was blood in her brain and the potential for deterioration,” Alouidor would explain later.
In the parlance of the trauma unit, this is what is known as a ‘category-2,’ or ‘cat-2,’ emergency, an incident less severe in nature than a ‘cat 1,’ which could be a serious motor-vehicle accident; a gunshot wound, or GSW, as one is called; a stabbing; or perhaps a paralyzing injury to an athlete.
But with either category, the message on the pager sets in motion a highly choreographed response that is part and parcel to life in the only level-1 trauma unit in Western Mass. When the patient arrives from CDH, the so-called ‘trauma team’ is ready and waiting to administer care that will continue long after the individual is taken from the trauma bay.
On this particular Monday, BusinessWest was a guest in the bay and surrounding emergency department to talk with team members about their work, its challenges, and rewards, and also record what would be considered a typical night in the trauma unit, although all those involved say there is no such thing.
Each day is different, said Alouidor, the attending trauma physician on this night, and unpredictability is the only constant.
Soon after the aforementioned patient, who suffered what’s known as a ‘mechanical fall’ arrives, the bay becomes awash in motion, with the various players — Alouidor, residents, a nurse, and others — attending to specific duties while trying to maintain order in what would be considered close quarters. There are a half-dozen people treating the patient, looking at information, and consulting with one another as data is pored over. In other instances, including most cat-1 cases, there may be two or three times that many people in the room (including security personnel and family members), necessitating what Alouidor calls “crowd control.”
“Having 10, 15, or even 20 people in the room is not unusual, and there’s a sign on the wall that identifies who is supposed to be there,” he explained. “It shows the room, it shows where the bed is, and it shows the position of each member of the team. As trauma-attending, when I have a very ill patient, I don’t just walk around the bed; I know where I’m supposed to stand — I have a position at the foot of the bed. My airway resident has a position at the head of the bed, the ED-attending has a position at the head of the bed, the trauma nurse and the trauma scrub nurse all have their positions marked out, they know where they’re supposed to be.
“So when we talk about choreography, or ballet, when we walk in the room, everyone knows their role,” he continued, “and everyone knows where they’re supposed to be.”
Life in the trauma unit is demanding, said those we spoke with, work that requires a broad mix of abilities, from the surgical skills needed to save lives to the soft skills one must possess to properly inform, comfort, and console patients’ family members.
“It’s a golden rule — the family needs to know what’s going on,” said Alouidor. “Even during resuscitation, family members have a right to be present, and someone from the team will detach from the team and stay at the side of that person so that they know what’s going on. If we admit a 4-year-old, the best medication I can provide to calm that child is his mother or father to hold his hand.”
Both tragedy and triumph, if it can be called that, can be found in the trauma unit.
“We make a lot of great saves here,” said trauma nurse Concetta ‘Chetty’ Jez, an evening supervisor in the emergency department and 38-year nursing veteran, who would emphasize that word ‘we’ with every comment she made about the trauma unit. “We don’t save everyone, but when you walk away, you’re thinking, ‘we really did it.’”
For this issue, BusinessWest talked at length with Alouidor and other members of the trauma team that night to gain a perspective on the choreography that goes on in the trauma unit, and how the ‘controlled chaos,’ as some described it, represents teamwork personified.
Step by Step
Alouidor, who was born in Zaire but is a citizen of Haiti and grew up in that country, told the BusinessWest that he’s always been drawn to emergency-room medicine and especially trauma care.
And in Haiti, where he did his first four years of surgical residency work, this care took on a different tone and tenor than what he would experience here later in his career, and provided different kinds of learning experiences.
“I come from a third-world country where our trauma systems are not as well as organized as here in the U.S.,” he explained. “Back home, we see things that you may have seen in the states 50 or 60 years ago, because at work, employees are not protected, and as a result, their hands get mangled in machines. Also, the streets are not properly lighted and the cars are not properly inspected, and as a result, you have a vehicle traveling with 20 people that was meant for 10, and when this vehicle tips over, everyone is injured.
“It’s a country where basic emergency services and transportation are not well-organized,” he continued. “So someone who has a car crash in a town 100 miles away from the capital is not stabilized and is brought to us by means other than an ambulance, and without having been properly screened or triaged. These are the patients that we had to take care of, so as a medical student, I was always very involved in the care of these patients and recall in my third and fourth year of medical school taking extra time to spend with residents in surgery so I could get more exposure to trauma.”
Alouidor would do a second surgical residency in New York City, and eventually came to Baystate in the summer of 2006. There, he spends roughly one-third of his time in what is the only level-1 trauma unit in the four western counties of Massachusetts — there is one at UMass Medical Center in Worcester and six in Boston — and one of three that serve Connecticut.
Level 1 is the highest designation for trauma units, and such facilities provde the highest level of care, said Dr. Ronald Gross, chief of Trauma and Emergency Surgery Services at Baystate Medical Center, noting that there are three levels of trauma facilities in Massachusetts, and as many as five in other states.
“If you take the overall spectrum of trauma, 100% of all injured patients, level-1 centers will care for about 15% of the trauma patients,” he explained. “All of the rest can be very well-cared for at community hospitals that are level 2 or less. The most severely injured patients should go to a level-1 center, and the statistics show that, if they do, you decrease their mortality by 25%. In fact, the numbers show that if you don’t take your patients to a level-1 trauma center and they go somewhere else first, mortality is four times that of those who go to a trauma center first.”
An emergency department is part and parcel of what is needed to have a level-1 trauma center, he continued, adding that trauma surgeons work hand-in-glove with emergency medicine physicians who staff the ER.
Key elements of a level-1 center include 24-hour in-house coverage by general surgeons and prompt availability of care in varying specialties, such as orthopedic surgery, neurosurgery, plastic surgery, anesthesiology, emergency medicine, radiology, internal medicine, oral and maxillofacial surgery, and critical care, said Gross. In addition, a level-1 center has a program of research, is a leader in trauma education and injury prevention, and is a referral resource for communities in nearby regions.
The long, severe winter of 2010-11 has added to what would be considered a typical workload in the trauma unit — again, if there is such a thing, said Gross. He noted that there have been more weather-related motor-vehicle accidents, by his estimation, a higher number of serious slip-and-fall incidents, and considerably more cases of people falling off roofs, an obvious result of the heavy snowfalls and homeowners’ attempts — almost always ill-advised — to reduce the threat of collapse. Meanwhile, Alouidor said this winter has seen a high volume of what he called ‘interpersonal violence’ — “there’s been a lot of penetrating injuries, a lot of gunshot wounds and stabbings” — a statistical anomaly he could not explain.
A recent serious head injury, a true cat 1, provides an insightful look at the full breadth of the work performed by trauma-team members after the pager goes off — and well after the patient leaves the bay.
“He had a very severe brain injury, and at the time of admission, we were all concerned about the potential outcome,” Alouidor recalled. “This patient put in a week in our ICU in which he received what we categorize as maximum medical therapy.”
Elaborating, he said that surgical teams moved quickly to decompress the brain, a procedure gaining more acceptance after recent success with soldiers in Iraq and Afghanistan.
“A large fragment of bone is removed, and thus the brain has room to swell,” he explained. “When there’s a brain injury, the brain’s main response is to swell, and with the swelling, the pressure in the brain increases, and that’s what leads to complications. There are multiple medications we can use to decrease the swelling and decrease the pressure and stabilize the patient, but this patient did not respond to any form of medical therapy, so at that point we had to decompress his brain.
“Despite this, his brain pressures were not properly controlled,” he continued. “After several days, he eventually died. We spent those days with the family, hand-in-hand with his wife, his children, his parents; it was a very long process, and a case that shows how we’re not just taking care of the patient, but taking care of the family.”
On the Clock
When asked what he enjoys (if that’s an appropriate word) about trauma work, Alouidor said he takes a great deal of satisfaction from making a profound and often immediate impact on someone who is probably having the worst day of his or her life, but there is much more to it than that.
“I like what I do for a variety of reasons,” he explained. “It’s not only the relatively quick results, but also the fact that I really like taking care of my patients; I’m very busy and very involved in their care, and that’s rewarding.
“There’s a wide range of results in trauma,” he continued, adding that not all of them come quickly, and some are obviously tragic in nature. “It’s not only the person who comes in in extremus that you can turn around very quickly by properly resuscitating them in the emergency room, bringing them to surgery, and doing the right operation at the right time, and watching this patient turn the corner within hours and come back to life; that’s the best-case scenario, but they’re not all like that.”
On the Monday he spoke with BusinessWest, Alouidor’s day began at 7 a.m., and the shift would continue until 7 the next morning. That might seem like a long shift to most, but he’s used to it — so much so that his body’s ‘clock’ is impacted when he’s not working. Indeed, he finds that, when he’s on vacation, by the time he’s a few days into a trip, or about when he’d normally be taking a turn in the trauma unit, he finds himself staying up all night.
Since this Monday was relatively quiet, Alouidor was able to spend some time with BusinessWest and discuss the many nuances of work in trauma. He said he arrives each day expecting “anything and everything,” and quite often gets both.
There is often no rhyme or reason to the level of the activity in the trauma unit, although there are some circumstances that will obviously contribute to volume, he explained, noting that the frequency of motor-vehicle accidents increases with bad weather and poor road conditions, and, in general, more bad things happen when people are outdoors, such as the summertime.
And there is, he maintains, scientific evidence of — and common-sense explanations behind — surges in activity during hot weather and full moons.
“The heat does things to people,” he said with a smile. “There is actually data in the literature that demonstrates that, when it’s a warm summer night or when the moon is out, trauma departments are more busy, and this is something we have known for years. When it’s warm, people are outside, and when they’re outside, things tend to happen — accidents, people fall off the balcony — and some bad things, like fights. And when you have a full moon, there is light until very late, and since people are out later, there’s more potential for them to get into trouble.”
And while this Monday was uncharacteristically calm — until mid-evening, at least — there are occasions, and many of them, he noted, when the patient volume on the first day of the work week will prompt someone to say, ‘are you sure today is Monday?’
Penetrating wounds, especially those related to interpersonal violence, have been occurring with great frequency this winter and, in general, over the past several years, said Alouidor, who noted that, had there been a shooting on the night of BusinessWest’s visit, he probably would not have been at liberty to talk about it due to health care privacy regulations. So he used a hypothetical situation to discuss these cat-1 cases and all the ways the trauma unit responds, starting with what his pager would be telling him when it went off.
Teaming with Anticipation
“It would be alerting us to a ‘category 1, GSW,’” he explained. “There would be an age to follow, a location of the wound or wounds — chest, body, head — and there be be vital signs, blood pressure, heart rate, mental status, and EMS can tell us if the patient is critical, meaning minimum vital signs, or stable.
“And stable is a relative term — young, healthy people can tolerate a lot before they crash, but when they do crash, they’re in trouble,” he explained, adding that ‘critical’ is a relative term as well, and one that refers to potentially life-threatening injuries and an individual who needs to be stabilized.
With the information from EMS in hand, the trauma team begins to mobilize, said Alouidor, noting that the information on his pager is also now in the hands of other departments and individuals whose services will likely be required. This list includes the ICU, the operating room, radiology, the blood bank, lab, and also pastoral care.
“We care for these patients, but also their families,” he said. “If someone arrives here and has their 25-year-old wife or 50-year-old mother or 17-year-old son with them, someone needs to sit down with these people and talk them through what’s going on. We’ll provide the necessary medical information, but they also need support; we want to make sure there’s someone there for the family if they need someone to talk to.”
By the time the patient arrives, the team members are ready, he continued, adding that, by this, he means they are gowned, masked, and fully prepared to perform the rapid assessment that is needed in such cases. Airway, breathing, and circulation are the first things checked, he said, adding that disabilities, mental status, and injuries are also assessed.
“I’m not distracted by the fact that someone has a hole in their chest and a hole in their abdomen and they’re screaming bloody murder,” he told BusinessWest. “What’s important to me is to see if the person is stable first, and then, in a very systematic fashion, we go over things. People look at us very cynically and say, ‘this guy’s been shot in the abdomen; why are you looking at the airway first?’ That’s because the first thing that’s going to kill this person is not the fact that they’ve been shot in the liver or in the blood vessels in the stomach. What’s going to kill them first is that they’re not breathing. What’s going to kill them afterward is the fact that they don’t have circulating blood.
“Then, we go on to assess the injuries and do what’s called a secondary survey,” he continued. “Then we make our decisions. Is this patient stable? Is he critical? Is this a patient we will do a workup on? This might be a gunshot wound we assess in ED and determine it’s not a penetrating injury. Then we can say, ‘it’s your lucky day; you got shot, and the bullet only grazed you,’ or ‘it didn’t go through any significant structures.’”
If the patient is critical and needs surgery, he or she is in the operating room within minutes, Alouidor went on, adding that other types of trauma, be they injuries from a car accident, fire, or fall from a roof, are assessed and treated in the same fashion.
And with every step in the process, the team is involved.
“I don’t work alone — I work with a team,” he stressed. “I could not provide the care I provide alone. And one of the reasons why modern trauma centers are so successful is not just because they have good doctors, nurses, X-ray technicians, or anesthesiologists. They are successful because they have good systems, and these systems are put in over months and years, and it is these systems that lead to good outcomes.”
Children make up a small percentage of the caseload in trauma, said Alouidor, adding that they bring some additional challenges to the fore.
Communication is one of them, he explained, adding that very young children can’t articulate what’s happened or where it hurts. “Parents can provide a story,” he explained, “but sometimes, that story is, ‘I was in the other room, I walked in, I saw him lying on the floor,’ so we don’t really know what happened in those circumstances. And to me, that’s one of the more challenging aspects of caring for kids.”
“Some people say it’s difficult to treat children because when you look at them you see your own children,” he continued. “And while that’s true, when I look at my patients, whether it’s the 20-year-old, the 45-year-old, or the 85-year-old, I tend to see someone I know. I think about my niece, who is 20 years old, I think about my brother, who’s 45, and I think about my parents. You tend to find yourself in any patient you’re seeing.
“It is more difficult to accept a child who has significant injuries, especially when you know the outcome will not be good, as opposed to someone who’s older,” he continued. “That’s not to say that you don’t care as much [with the older individual], but it’s easier to understand and cope with someone who’s 88 and coming to the end of their life than it is with a child who’s 4 who has a devastating injury and will live with those complications for the rest of his life.”
Work in Progress
‘The Q word.’
That’s the usually unspoken term for ‘quiet’ in the trauma unit — and in most hospital settings, for that matter.
Those who are superstitious won’t say it out loud, said Dr. Mazen Al-Mansour, a surgical resident at Baystate who spends good deal of his time handling trauma work. That’s because doing so will, in their minds, inevitably change the course of an otherwise calm evening in the bay.
Al-Mansour is a fourth-year resident in the Department of Surgery, which means he’s nearing the end of this long, grueling stretch of his training. He told BusinessWest he would like to become a general surgeon, but enjoys many aspects of trauma work, especially the pace and unpredictability of the work.
When asked if organized, or controlled, chaos would be a good way to describe what goes on, he said only those who don’t work in the unit would use that term, even if it is fairly accurate.
“Everyone knows exactly what’s going on and what’s going to happen next, when there are multiple traumas at the same time or when we get extremely sick patients,” he explained. “It can be a little chaotic, but that’s the nature of traumas.”
Echoing Alouidor, Al-Mansour said work in the trauma unit requires a mix of skills, from the ability to assess and treat a penetrating wound to the compassion needed to address the wants and needs of family members.
“We work closely with extensively trained trauma surgeons who have the experience of dealing with life-threatening injuries in different areas of the body and different kinds of trauma, such as penetrating trauma or blunt trauma such as a motor-vehicle accident or people who are struck by vehicles,” he said. “We get to work closely with these people — we get to be the first-assist when it comes to the operation, and we get to watch these people talking to families, and we get to be involved with the families as well.
“There are different levels of people who get involved, and different levels of experience,” he continued, “and a lot of mentorship and observation on the part of younger people to pick up on the skills and the knowledge of how to handle the trauma patients and their families.”
Jez, whose job it is to coordinate nurse activity in the emergency department, including the trauma unit, said trauma nurses are specially trained for their work, which is demanding physically and also emotionally, but in many ways rewarding.
“It’s one of the greatest places to work in, and the nurses, while they can feel stressed — it’s a very, very busy place — will say that they truly make a difference,” she said, adding that the nurses play a critical and yet often overlooked role in the ED and the trauma bay.
“When these patients come in to the trauma unit, there’s this huge hurry — everyone’s in this big rush, everyone’s all excited, and the adrenaline’s flowing,” she explained. “And the nurse is in the middle of it. It’s the nurse and the patient, it’s the nurse who brings in the family, it’s the nurse who does all the meds, it’s the nurse that’s doing all the re-evaluation, it’s the nurse who’s there when you’ve lost the patient, and it’s the nurse who makes the patient look presentable so the family can come in and see him.
“They do it because it they love it,” she said of the nurses and their work. “They cry a lot down there — that goes with this territory — and they find order in the chaos.”
Alouidor stressed repeatedly that ‘quiet’ — he’s not at all afraid to use the ‘Q’ word — doesn’t translate into not busy.
Indeed, trauma physicians have patients to continually evaluate and myriad other types of work to handle when beds 9 and 10 in the trauma unit are empty or emergencies have passed. And they know that, at any minute, even if the moon isn’t out or it’s warm outside, the pace of the evening can change dramatically — and often does.
That’s why there are systems and procedures and signs on the walls in the bay telling people where to stand. The only job description for the people who work in this unit is to be ready — before the pager alerts them to an arriving patient, and long after the controlled chaos begins.
George O’Brien can be reached at [email protected]

Joint Replacement Makes Significant Strides

Dr. Henry Drinker says demographic trends and improvements in technology have combined to cause an exponential rise in the number of patients receiving new hips and knees.
Total joint replacement has long been considered a surgery for older, not younger, people — but not too old.
The rules, however, are changing.
“It’s mainly for arthritis, and arthritis is an age-related condition; most patients have been in their middle-aged years, some of them elderly,” said Dr. Henry Drinker, an orthopedic surgeon at Hampshire Orthopedics & Sports in Hatfield. “But more and more, we’re treating a younger patient population, due to a host of factors, including an increased emphasis on athletics and physical fitness, which has produced a lot of arthritic knees in younger people.”
Dr. Robert Krushell, medical director of the Hip and Knee Replacement Program at Baystate Medical Center, said the age of likely candidates for joint replacement has expanded on both sides of the spectrum.
“It’s common to see people coming into the office in their 50s, and sometimes younger than that, who need hip or knee replacement. And with the technology we have today, we’re much more comfortable offering it to people in that age range because it will last longer,” he said.

Dr. Robert Krushell says the age of likely candidates for joint replacement has expanded on both sides of the spectrum.
Those two trends point to one unmistakable fact: joint replacement is a very healthy field in which to practice today, with about 350,000 total knee replacements and close to 200,000 hip replacements being performed every year in the U.S., Drinker said. “And it’s on an exponential rise, partly because of Baby Boomers coming of age and experiencing arthritic joints.”
And that trend — both locally and around the country — is projected to continue over the next two decades, said Krushell. “Current projections say that the number of people getting hip replacements per year will double 10 years from now, and knee replacements will triple.”
Fortunately, doctors say, the technology that enables total joint replacement has improved, and the materials used have become more durable, to the point where the risk of complications has become much less for older patients, and artificial joints last much longer in people who undergo the procedure at a young age.
“There has always been a big concern about taking a damaged hip or knee in a young person and replacing it,” Drinker said. “You were pretty much guaranteed that the procedure would have to be done again in 15 or 20 years, or less, and redo procedures are much more invasive and much more destructive. So evolutions in the field have made it possible to bring this to a greater number of patients with joint problems.”
This month, BusinessWest takes a look inside the changing world of total joint replacement and the advances that have made the surgery safer, and the results longer-lasting, just as more and more Americans of all ages are clamoring for it.
Hip Knee Hooray
The practice of joint replacement can, and does, encompass shoulders, elbows, wrists, and hands, but the vast majority of cases involve hips and knees.
The procedure is essentially what it sounds like: removing a damaged joint and replacing it with an artificial one, usually made from plastic or metal. The materials may be cemented into place, or not cemented and instead designed for the bones to grow into the prosthesis; the latter tends to have a longer recovery time, but also lasts longer in the long run, often making it a better option for younger people.
Dr. Khalid “Kelly” Instrum, an orthopedic surgeon with Holyoke Medical Center, said patients, along with their doctors, make the decision to undergo total joint replacement based partly on how their arthritis or other condition affects their ability to partake in day-to-day activities.
“For a younger person, that might be their athletic ability, while for an older person it may be the ability to take a walk with their spouse. Joint surgery is purely elective, and it depends on how it affects them. We never tell people they have to have it; it doesn’t save their life, but what we do does improve their life. As long as someone is healthy enough to go through surgery, it is pain-relieving, and something that gives people their lives back.”
In recent years, Krushell noted, new bearing surfaces have been developed that wear much more slowly and withstand much more activity without excessive wear, increasing the projected lifespan of these implants. The cementless option is particularly exciting, he said.
“There’s no longer any glue to loosen over time. These bonds that the bone makes onto the implant seem extremely durable; we almost never see these hip implants loosen. It’s a radical change, and we’re hopeful that some of these implants will be bonded to the bone forever.
“In the area of knee replacements,” he continued, “we’ve seen similar improvements in the area of bearing materials, and we’re just starting to delve into using knee replacements that also don’t need bone cement in the hope that, just like hip replacements, we’ll find that knee replacements get more permanent bonding. That’s pretty new, cutting-edge technology for knee replacement that’s not being used much around the country, but it’s starting to slowly gain traction.”
Instrum has also observed a series of evolutions in the field, from new materials to the increasing use of minimally invasive surgical techniques.
“We can make smaller incisions without cutting the muscles, so the length of stay after surgery is reduced,” he said. “It allows people to get up and get going quicker. With the techniques we used to use, people had to watch how they bent over after hip replacement, but with modern techniques, often they don’t have to worry about those types of problems anymore.”
Drinker noted that, with minimally invasive methods, “the ease of recovery may be affected, and the pain to the patient is maybe less. Scars are smaller, and blood loss is lower.”
Still, he said, such surgeries are not standard across the discipline. “They have a steep learning curve and are fraught with complications. There will always be some surgeons who use these techniques, but I’m not sure they’ll be universally recognized everywhere.”
In addition to the emergence of minimally invasive surgery, allowing patients to recover more quickly, Krushell said, “another thing that’s been very helpful is some of the newest techniques in post-operative pain control. It hurts a lot during the first few days after surgery, but if you have good pain control, it can be a lot easier to get up and out of bed, do your therapy, and get good motion in your joint.”
Progress Around the Bend
Drinker, who is affiliated with Cooley Dickinson Hospital, touted CDH’s dedicated Joint Replacement Center as the wave of the future in this field.
“What we have here at Cooley Dickinson represents the state of the art,” he said of the 12-year-old department; before that, joint-replacement patients were part of the general hospital population. “In this segregated physical space in the hospital, those patients are the only patients on the floor. It’s almost a quarantined unit in the hospital, and it’s had a big impact on patient experience and outcomes. I believe it’s the only dedicated total joint service in New England.”
The primary advantage, he said, is that all nurses and physical therapists on the floor are trained in the subspecialty of joint replacement. Not only is the patient-nurse ratio small, but patients can expect a certain consistency of care since they aren’t being treated by nurses rotating in from other units.
“What’s really special about the joint center is that we have a specialized program for joint-replacement patients. We have a separate unit, and we have our own exercise room right here in our unit, and we have a pathway of care specifically for joint patients,” said Anne Ridabock, clinical coordinator of the center. “We try to do most joint surgeries on Mondays, then 99% of the time they’re discharged on Thursday. And they can follow this path together: group exercise every day, as well as individual exercises tailored to them.
“Our staff here is just so well-versed in caring for joint patients; they’ve undergone specialized training and have years of experience as well, and that makes for a very smooth, very efficient process,” she continued. ”The patients are continually telling us, ‘you work as a team here; you anticipate what we need.’ It’s an amazingly smooth operation.”
The setup also helps to control complications, particularly infections, Drinker said, noting that the national infection rate for joint-replacement surgery is about 1.5%, while Cooley Dickinson’s is around 0.6%. “One reason is that, by having a quarantined floor, these patients are not subject to hospital-borne infections to the extent they would be on a general medical floor.”
Ridabock said the unit’s focus on “going the extra mile” in infection control includes the hospital’s recent adoption of a cutting-edge system that disinfects patient rooms using ultraviolet light. “And all joint-replacement patients have to be cleared of infectious processes, because an infection in the joint is a real problem. Just having a specialized unit keeps complications low, patient satisfaction high, and really aggressive physical therapy possible.”
Having a specially trained nursing staff also cuts down on the incidence of dislocation in the first few days following the procedure, Drinker added. “The occurrence of a dislocation in the first few days after this operation is often related to nursing care and patient education.” Meanwhile, he added, group-therapy sessions allow patients to share each other’s apprehensions and triumphs.
One Step at a Time
Doctors share in such triumphs, too, and Instrum said it’s gratifying to see people able to do more things, whether it’s a young or middle-aged patient or a Baby Boomer who — like many members of that generation — intend to stay vigorous well into their retirement years. “Obviously it’s good for their general health and helps them be active.”
Krushell cited a patient who went on to achieve long-time goals, including visiting the Grand Canyon and the Great Wall of China. “She never thought she’d be able to do stuff like that. Then a lot of patients just say they want to go for walks with a parent or grandparent.”
Helping them get there, he said, is personally satisfying.
“I feel amazingly blessed to be in my field. In my normal day in the office, I see people starting to get their lives back again. People commonly say this is the best thing they’ve ever done, so it is very gratifying to see people who couldn’t get around before surgery get back to their lives again.”
Joseph Bednar can be reached at [email protected]
Keeping Health Care Reform on the Front Burner
No single reform would do as much to improve the wealth of our nation and the lives of Americans as a comprehensive overhaul of our health care system. But the best chance of swift and major reform may have died with the end of Hillary Clinton’s run for the White House.
Sen. Clinton kept health care on the front burner, promising action in her first term. Health care has already slipped as the top domestic concern, a position it held earlier in the campaign for the first time since the last Clinton campaign in 1992. The economy has passed it. But you can’t have a healthy economy without a functioning health care system.
Unfortunately, there are no easy fixes, no simple wands that can be waved to solve what ails our health care delivery system.
America should be the envy of the world when it comes to delivering health care, since we pay more per capita than any other nation, soon nearly 20% of our gross domestic product. In many areas of medicine, particularly in research, we are leading the world. But in others, we are not keeping pace.
We have the second-worst newborn-mortality rate in the industrialized world, and rank highest in preventable medical errors. Even worse, one in six Americans has no access to high-quality medical care. What we need from the next president is real leadership and a vision for changing what’s wrong with our health care system.
Sens. John McCain and Barack Obama have reform plans that take divergent paths, neither of which is as comprehensive as Clinton’s. Obama would require that children have health coverage, but not adults. The problem with that is, if there is no mandate for adults, the young and the healthy will opt out, leaving the older and sicker in the system. This would likely force premiums up.
Obama takes a page from the Massachusetts health-reform law and would require employers to offer ‘meaningful coverage’ or contribute to a new public plan for the uninsured and small businesses. He also says health insurance would be more affordable with lower co-pays and deductibles, and he would require insurers to offer coverage without exclusion for pre-existing conditions. He would also allow those without insurance through an employer to buy into plans now available to some federal employees.
McCain’s plan follows the Republican playbook, that the answer is to cut costs and inspire all Americans to buy insurance by means of tax incentives. His plan would end the tax deduction that employers get for their share of employees’ premiums, thus undercutting the employer base of most families’ insurance. Instead, he would give families a $5,000 tax credit toward any coverage they buy.
The McCain camp says the tax credit should encourage insurance companies to develop plans that come in at that price, no easy task in high-cost states such as Massachusetts. He would encourage competition by allowing insurance to be sold across state lines.
Both plans fall short, and neither truly promises universal access. McCain’s plan is particularly radical in that it would eliminate the ‘safety net’ that employees have come to value and would undoubtedly put more of the cost of health care directly on individuals and families. Furthermore, individual insurance sold on the open market is inevitably more inefficient for insurers and more expensive for consumers. It may make it harder for those with chronic conditions to get health insurance.
There are three areas the next president must focus on, and all three must be in balance: making sure every American has health insurance, improving the quality of care, and controlling costs. Viable solutions to our nation’s health care crisis will require a bold plan for action, not rhetoric. We can thank Clinton for driving that point home. Whether her health plan was right or wrong, she was tenacious and brave, and her plan was the most comprehensive and detailed. We should demand the same from McCain and Obama.