Bridging the Gap
By Emily Thurlow

With classic Christmas carols softly emanating from a TV across the room and an Irish wolfhound named Veren panting rhythmically a short distance behind her, Barbara Chiampa pedaled a stationary bicycle on a recent afternoon at Mont Marie Rehabilitation & Healthcare Center’s therapy gym.
With guidance from Reliant Rehabilitation physical therapy assistant Tara McCauley, Chiampa was working on improving her balance and walking. After noting improvement in her gait and movement with a handheld assist, Chiampa paused for a few kisses from Veren, a 2-year-old therapy dog.
The staff at the Holyoke facility benefits from the canine too, said his handler, registered occupational therapist Sylvia Korza of Reliant Rehabilitation. “He comes to work with me, and he loves everybody. He’s great for therapy — even the staff. He helps lift everyone’s mood.”
The gym, which was expanded in 2016, features several pieces of equipment dedicated to improving mobility, including parallel bars and practice stairs. Beyond the machines, the therapy gym offers opportunities for McCauley and Korza to customize regimens that are tailored to the specific needs of patients recovering from medical procedures, injuries, or illnesses.
The therapy offered at the center’s gym is one of multiple subacute rehabilitation care services offered at the 84-bed Mont Marie facility, which was built in 1962 and formerly owned and operated by the Congregation of the Sisters of St. Joseph. In 2014, Mont Marie was purchased by Tryko Partners, which is headquartered in New Jersey, and is managed by its healthcare subsidiary, Marquis Health Consulting Services. Mont Marie is one of 10 of Marquis’ facilities in Massachusetts.
In recent years, the licensed nursing facility’s short-term rehabilitation care services have continued to grow, adding new programs and certifications, to meet the growing needs of the community.
A need for subacute or short-term rehabilitative care can emerge after a hospital stay for hip surgery or a stroke, or if an individual needs some physical strengthening or medication management, said Natasha Pieciak, administrator at Mont Marie.
“Baby Boomers are getting older, so as the population ages, there’s more of a demand for supportive services. We’re not a hospital — we’re kind of like a step down; we’re supportive services to bridge that gap between home-care services and the hospital.”
Initially, the 26-bed first floor was dedicated to this service, but it has since expanded to the 29-bed second floor as well. At times, admissions have jumped as high as 50 per month.
“There are a lot of factors that influence this growth,” said Pieciak, who has served as administrator of the center since September 2022. “Baby Boomers are getting older, so as the population ages, there’s more of a demand for supportive services. We’re not a hospital — we’re kind of like a step down; we’re supportive services to bridge that gap between home-care services and the hospital.
“With the aging population, I think these services become more needed out in the community, so we’re here to support people in that way, so they can be successful at home. People want to be at home, so we’re really here to try to support them to get them ready to do that.”

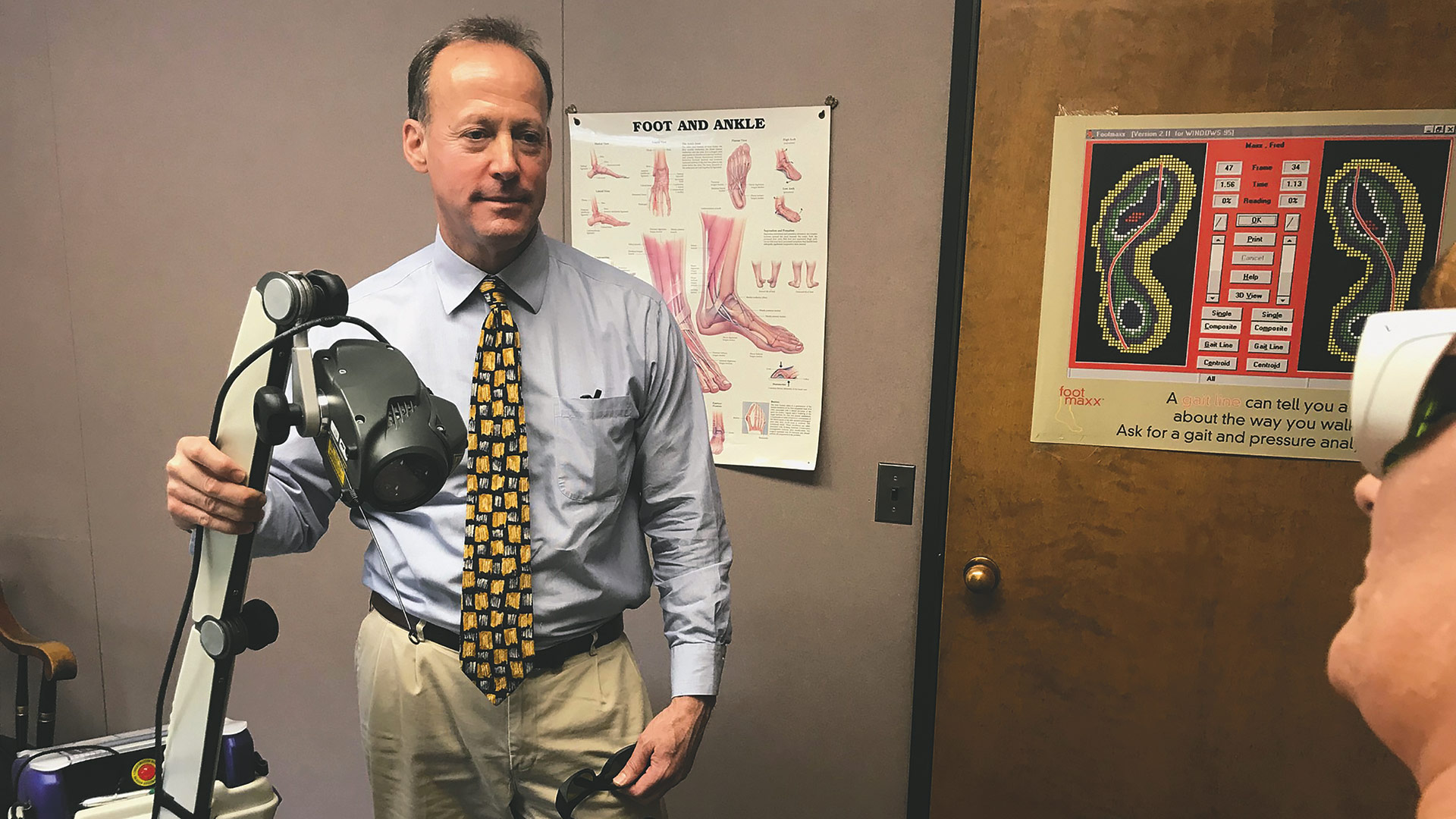
Barbara Chiampa pedals an exercise bicycle at Mont Marie Rehabilitation & Healthcare Center in Holyoke.
Through Mont Marie’s partnerships with Baystate Medical Center in Springfield and Holyoke Medical Center, as well as referrals from Mercy Medical Center in Springfield and Cooley Dickinson Hospital in Northampton, Pieciak said Mont Marie has been made aware of the growing demand for these rehabilitative services.
“We work closely with our partners within the hospital systems; we collaborate,” she said. “With Baystate, for example, we have weekly calls with their accountable-care organization management team, who will follow a patient from hospital to home, and we communicate with them, and they tell us what they’re seeing, what their needs are. We’re just really building that relationship and working with them to help identify and meet the needs that we’re seeing out in the community.”
“The goal of these specialty programs is to educate and train the residents how to manage and live with their conditions.”
In working with Baystate, Pieciak said Mont Marie has become one of two skilled-nursing facilities that have qualified for a waiver for the three-day requirement under the Medicare Shared Savings Program. The waiver eliminates the requirement to have a three-day inpatient hospital stay prior to a Medicare-covered, post-hospital, extended-care service.
What this means, Pieciak explained, is that, if a patient is in a hospital emergency department but don’t have a three-day stay, instead of going back home and potentially falling or fracturing a hip, they could go to Mont Marie as long as they meet a skilled need.
“This is huge because there’s a gap there,” she said. “Residents would go home and could potentially have worse outcomes. What we’re doing is bridging that gap from hospital to home.”
In addition to physical and occupational therapies, Mont Marie’s subacute rehab offers speech therapy up to seven days a week.
Life Goals
Within its major focus on subacute rehabilitation care, Mont Marie offers three specialty programs: cardiopulmonary, chronic kidney disease management, and heart failure.
“The goal of these specialty programs is to educate and train the residents how to manage and live with their conditions,” Pieciak said.

Natasha Pieciak says Mont Marie works closely with its partners within hospital systems.
The cardiopulmonary rehabilitation program is physician-led under the direction of a pulmonologist and focuses on helping patients achieve the most active life possible despite any physical limitations and/or cardiopulmonary diagnoses. The program, which is geared toward individuals with diagnoses of chronic obstructive pulmonary disease (COPD), post-lung transplants, emphysema, and acute respiratory failure, offers access to lab and radiology services, tracheostomy care and management, nebulizer therapies, bladder scanning, and several oxygen therapies, including liquid nitrogen.
The renal program is focused on reducing symptoms of chronic kidney disease, increasing a patient’s quality of life, and promoting independence. Mont Marie offers onsite dialysis provided by American Renal Associates, consultative visits by staff nephrologists, diabetic management and education, a monthly support group, and health coaching.
In October, Mont Marie received its skilled-nursing facility heart-failure certification from the American Heart Assoc. (AHA). In order to be considered eligible for this certification, facilities must be located in the U.S. or a U.S. territory and implement a heart-failure program that uses a standardized method of delivering clinical care based on current evidence-based guidelines.
“This was a huge accomplishment,” Pieciak said. “There are very few facilities that are credentialed. The American Heart Association has armed us with innovative methods and additional tools so that we can be trailblazers and give our heart-failure patients the best care.”
The vetting provides an evidence-based framework for evaluating skilled-nursing facilities against the AHA’s science-based requirements for heart failure patients, including care coordination, clinical management, quality improvement, program management, and patient and caregiver education and support.
According to the AHA, nearly one in four heart failure patients are readmitted within 30 days of discharge, and approximately half are readmitted within six months. It has also been suggested that about 25% of readmissions may be preventable.
“We’re trying to get ahead of hospital readmissions,” said Raymonda Sample, the lead for the heart-failure program and unit manager.
With the certification, Mont Marie has been provided with access to centers on treating heart failure and its co-morbidities.
Sample noted that one of the biggest benefits to the staff’s education on the heart-failure program is being able to educate patients on how they can live more independently with fewer flareups of their disease.
To that end, Mont Marie uses what’s called a ‘zone tool.’ The traffic-light color-coded guide indicates an all-clear, or green, when a patient has no shortness of breath; chest pain; swelling of the feet, ankles, legs, or stomach; or weight gain of more than two pounds. It’s time to call a doctor if a patient is in the so-called warning (yellow) zone, when they’re experiencing dizziness; dry, hacking cough; more shortness of breath; uneasy feelings; no energy; difficulty breathing when lying down; swelling of the feet, ankles, legs, or stomach; or weight gain of three or more pounds in one day or five pounds in one week.
A medical alert, or red zone, is when the previous symptoms have been exacerbated and a patient is having a hard time breathing or is experiencing unrelieved shortness of breath while sitting still, chest pain, or confusion.
In addition to this tool, Sample has created an entire guide board for staff that she also uses to educate family members of patients. The tool helps provide a better continuity of care, she explained.
“With this education, we are able to identify how the patient is feeling for the day,” she said. “If say, the patient is in the middle of therapy and they’re feeling short of breath, or telling the therapist maybe they haven’t eaten much in the last couple of days, or not sleeping well — there’s a sort of board out there where you can see the different signs and symptoms of heart failure.”
Safe at Home
Even though a patient has a plan in place to be discharged from the facility following treatment at Mont Marie, care doesn’t end at the door.
“When we discharge patients, we do follow-up calls with the patient just to find out how the transition back home goes, the home care services … we make sure they’re seen by their primary-care physician within 10 days, and if they don’t have a scale, we make sure we send them home with one,” Sample said. “This is so both our patients and the staff recognize the signs and symptoms of heart failure, so we can try to avoid rehospitalization.”