Living in Their World

Beth Cardillo calls them ‘fiblets.’
These are things that are said to someone with dementia that … well, do not represent the whole truth, or even a portion of it, at least to the person making that statement.
But to that person suffering from Alzheimer’s or one of the many other forms of dementia, it is the truth as they see it in their world. “It’s not a lie,” she said of these fiblets. “It’s an OK thing to tell people with memory issues.”
She offered up an example.
“Let’s say someone’s husband has been dead for 20 years; she might say, ‘I’m not going out shopping, I’m waiting for my husband to get home,’” noted Cardillo. “A fiblet would be … ‘oh, he just called; his tooth is hurting him and he’s going to see a dentist. Why don’t you and I go out for a ride and go to the grocery store?’”
“You’re going to tell someone that their husband died over and over again, every day?” she went on, asking that question rhetorically before answering it poignantly. “I mean, why would I want to do that? It’s cruel.”
Indeed, and fiblets are a good example of how those caring for and simply around individuals with dementia regularly should try to live in their world, rather than constantly try to pull them into the ‘real’ world. It’s also an example of the kind of work that Cardillo has made into a career, or at the least the latter stages of one.

Beth Cardillo
Her latest move comes as a part-time social worker for a unique program called Baystate House Calls. As that name suggests, it’s a program operated by Baystate Health that involves healthcare professionals making house calls to older adults. It includes a physician, nurse practitioner, nurse, social worker, and community health worker, team members who will visit individuals in their home to assess their needs and provide recommendations.
The initiative concentrates on what administrators call the 4Ms — ‘mobility,’ ‘what matters,’ ‘medication,’ and ‘mind.’
It focuses not only on those in need of help and services, but caregivers as well, said Cardillo, adding that her work, and that of her colleagues, takes them to every corner of Springfield. And while she is helping seniors and caregivers with a wide variety of issues from substance abuse to falls to depression, much of her work involves those with memory issues.
And, increasingly, it involves what is known as habilitation therapy (HT), a holistic approach to dementia care that focuses on the abilities that the person still has, rather than what they have lost, and can reduce difficult symptoms.
“It focuses on everything positive — it focuses on people’s strengths, not their weaknesses,” she said of HT, adding that it brings caregivers and patients closer together as they work on daily tasks, makes those suffering from dementia feel respected and valued, reduces stress among caregivers, and creates positive emotional experiences that bring comfort and happiness.
“The reality therapy is for us to learn to live in their reality, not for them to live in our reality of our world. That’s probably the biggest lesson there is.”
Cardillo was recognized by BusinessWest and its sister publication, HCN, with a Healthcare Heroes Award in 2021 in the category of Community Health for her work during her years as executive director at Armbrook Village in Westfield to create ‘dementia-friendly’ communities and help others better understand — and communicate with — those suffering from memory loss.
For this HCN Monthly Feature and its focus on Memory Care, we talked with her at length about the importance of understanding what is reality that for those with dementia — and enabling them to thrive, as much as possible, in that reality.
Reality Check
Cardillo told BusinessWest that, years ago, she and others involved with providing memory-care services would offer to those with dementia what was called, by some at least, ‘reality therapy.’
“We would say, ‘no, no, no, you’re wrong — today’s Thursday, or today’s this, and tomorrow is that,’ she said, correcting wrong statements and answers to questions whenever the need arose. “But what we’ve learned is that it doesn’t matter. The reality therapy is for us to learn to live in their reality, not for them to live in our reality of our world. That’s probably the biggest lesson there is.”
Helping others live in the reality of those with dementia is a big part of the work Cardillo has been involved with over the years, especially at Armbrook, but also now as a social worker. She said that to make this leap — and it is a leap for most — it begins with education and an understanding of the disease and how it impacts people.
It robs them of short-term memory and the ability to do certain things — from driving to cooking to reading. But it doesn’t, or shouldn’t, take from them the things that are important to them, and have been important throughout their lives, be it what they did for a living, or travel, music, pets, or a love of the movies.
Cardillo recalled the case of a long-retired college professor who had (and still has) a passion for the New York Times and carries it with her daily.
“Some days, it’s upside-down,” said Cardillo. “But it doesn’t matter; that was her identity. Those are they types of things you don’t want to change; you don’t want to correct people.”
Overall, she said it’s important to treat those with dementia with respect and to not embarrass them with ‘reality’ questions or constant corrections concerning what day it is and what members of the family are no longer alive.
“It doesn’t matter if they say it’s Tuesday and it’s really Sunday. It just doesn’t matter. So, we don’t want to correct people. Does it matter if Mr. Smith thinks it’s a different day? Is that going to change the world? No. If he thinks it’s Christmas tomorrow, that’s OK. Why take that joy away?”
“Just because you have Alzheimer’s doesn’t mean you’re stupid,” she explained. “It doesn’t mean you can’t read people’s emotions. “I know people who will say to family members, ‘what’s my name? What’s my name?’ Why are you saying that to them? It embarrasses them. They know you have a connection. Is it because you think that if they know your name, they’re having a good day and that makes you feel good?
“Because it doesn’t matter if they know your name,” she went on. “It doesn’t matter if they say it’s Tuesday and it’s really Sunday. It just doesn’t matter. So, we don’t want to correct people. Does it matter if Mr. Smith thinks it’s a different day? Is that going to change the world? No. If he thinks it’s Christmas tomorrow, that’s OK. Why take that joy away?”
She recalled the case of a woman who told her that she was pregnant at 66. Instead of correcting her, Cardillo said she simply told her, ‘if that’s true, you’re going to make history.’
“You laugh about it with her, because she tells me these wacky stories,” she went on. “Her parents have been dead, but she’ll say, ‘oh, my mother wants you to come over for dinner.’ “I’ll say, ‘oh, how is your mother? I like your mother; tell her I said hello.’
“Her husband, on the other hand, keeps saying, ‘your mother is dead!’” she continued. “We need to stop that because it doesn’t matter. She doesn’t remember and she doesn’t care, and in in her head, her mother is alive. That’s fine. Who does it hurt?”
Overall, she said it’s important to try to communicate with a positive spin, rather than a negative one.
Indeed, instead of telling someone with dementia that they are not supposed to be going outside, when they suggest that they want to do so, one should instead stay positive and suggest that this person can sit outside when the weather is better.
As she talked about those suffering from dementia and how those caring for them should approach daily conversation and activities, Cardillo said it is important to keep them engaged and to focus “on what they can do, not what they can’t do.”
This brings her back to the concept of habilitation therapy, which, she believes, has benefits, and many of them, for those living with memory loss, their caregivers, family, and friends.
“It’s important to keep people meaningfully busy and not just silly busy,” she told BusinessWest, adding there is a big difference between the two.
Elaborating, she said that television is not a good option.
“We don’t want to put people in front of a TV all day, because it’s … not good,” she said. “It doesn’t make them happy campers. It doesn’t mean that TV is bad, just not as a babysitter all day.”
Instead, such individuals should be involved in activities that speak to who they are, who they were professionally, and what interests them.
“It’s really important to know what people did in their work,” she explained, “because they still retain some of those skills, and it’s still a part of who they are as an identity. For those who were teachers, give them papers to correct; you come up with things that they can do.
“I had someone whose father was a retired electrician,” she went on. “He had a manual of electrical … something; it was bigger than the New York City phonebook. He looked through those pages every day. I don’t know if he knew what was in it — I sure didn’t — but that gave him comfort.”
And some form of comfort is what those caring for people with dementia should be trying to provide each day, she said, adding that this can be done through HT, emphasizing the positive, and, yes, focusing on what those with dementia can do, not what they can’t.
Bottom Line
Summing up what she tells those caring for people with dementia, Cardillo said it is simply that reality is in the eyes — and mind — of the beholder.
And if we really want to help those with this disease, we have to at least try to live in their world, rather than make them live in ours. It’s not an easy assignment, especially when one is asked the same questions over and over, day after day, but it’s the key to those on both sides of the equation being able to thrive.





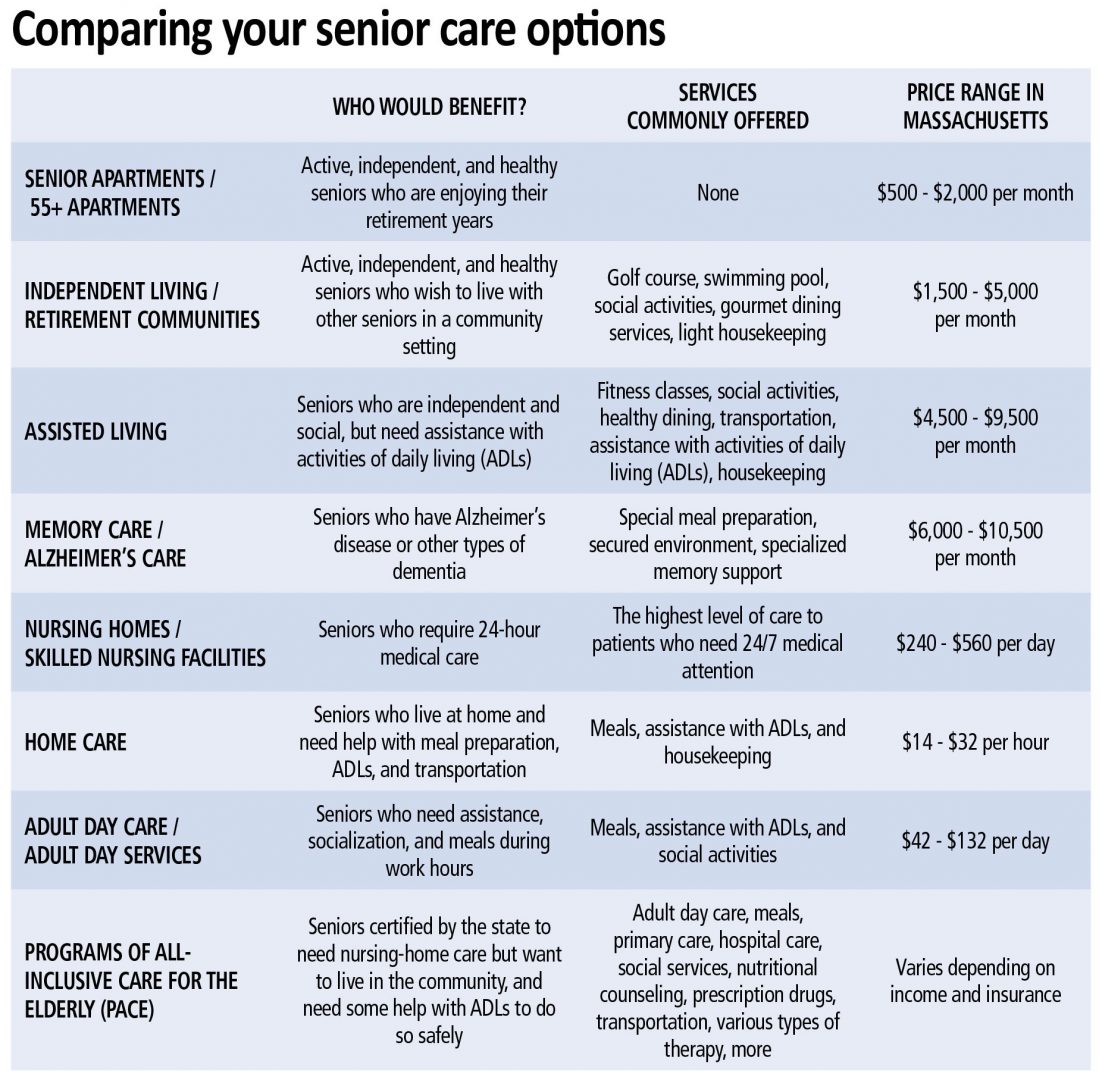
 By the Massachusetts Senior Care Assoc.
By the Massachusetts Senior Care Assoc.