Re-connecting the Dots of Life
By Alta J. Stark
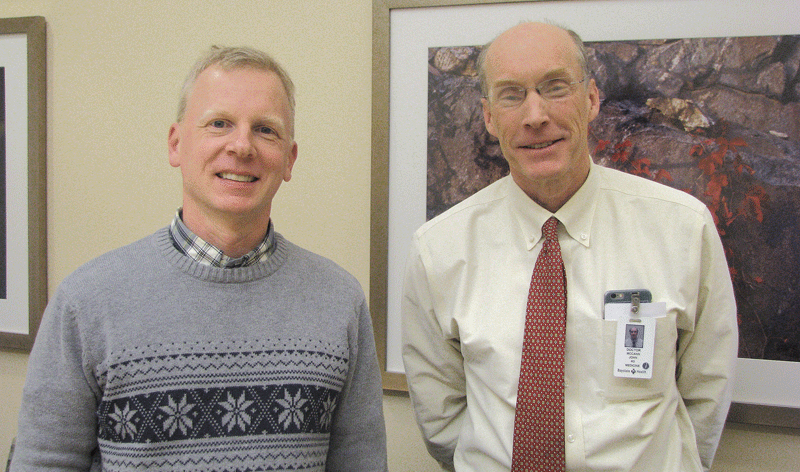
From left, Beth Cardillo, Terry Hodur, and Susan O’Donnell.
Helen S. is in her 80s. She’s lived at Armbrook Village Senior Living Residence in the northwest corner of Westfield since June 2016.
A resident of the community’s assisted-living homes, she receives help with many activities of daily living. When Helen moved here, she exhibited many of the cognitive challenges of aging, which can range from basic memory loss to Alzheimer’s disease. She would stay in her room and watch TV. Aides would guide her to and from meals and visit with her, but Helen didn’t socialize or make friends with other residents.
A long-time friend of hers, Terry Hodur, says she was getting discouraged. “There was a care meeting about a year ago when we discussed how quiet and reserved Helen had become. She would never step out, and she would always say ‘that isn’t my business,’ and she would turn away from people. It seemed like there was no way to help her, and we were told we needed to prepare ourselves for a possible move into the memory care unit.”
Then, Beth Cardillo, the residence’s executive director, mentioned a new program that was getting underway at Armbrook called ConnectedLIFE. The program is designed to meet the unique needs of those beginning to show signs of dementia.
“They might not process as quickly as they used to, or maybe they don’t remember things like how to play a card game, or people’s names, so they tend to isolate themselves in their room; they don’t engage in social activities and they tend to become depressed, frustrated and angry,” she explained. “This program helps them maintain connectedness, independence, and confidence.”
A few weeks after Cardillo mentioned the program, Helen started participating, and soon, Hodur saw a transformation she says is nothing short of amazing.

Helen S., Terry Hodur’s formerly shy, reserved friend, enthusiastically took part in a tea party for Queen Elizabeth’s 90th birthday at Armbrook Village.
“She’s doing well and she’s so happy,” said Hodur. “The ‘aha’ moment for me, came one night after dinner when Helen left her walker by me and walked over to a woman in a wheel chair who could really benefit from someone helping her, and Helen just started to push her into the room where residents gather. When she came back to me, I said ‘Helen, that was phenomenal,’ and she said ‘what do you mean? Of course I was going to do that!’
“To me, that was just a giant step,” Hodur went on. “This very quiet, reserved person is now someone who jumps in to help her friends. She wasn’t going to breakfast, now she is; she was losing weight early on, and now she’s starting to gain it back. ConnectedLIFE is providing a significant service, helping people like my friend Helen.”
Life’s Work
Susan O’Donnell, a certified dementia practitioner, is the director of the ConnectedLIFE program at Armbrook, and she explained how it came to be.
“We noticed that many of our assisted living residents were wandering around the building and not going to their preferred activities. They didn’t really have anything to do, and wouldn’t get up til noon, or one o’clock in the afternoon. So we designed a specific program that not only jumpstarts their days but also meets their therapeutic goals. It’s a set of failure-free activities that provides just the right challenge for them to be successful.” O’Donnell says the program is an intimate peer group of people who have a lot in common.
“We try to foster fun and laughter, because laughter is a good medicine. It’s one of the brain chemicals that get released and when you laugh, it makes you feel good,” she told BusinessWest. “We also talk a lot about relationships and reminisce, because these women (the group is presently all women) have a lot of things in common, and they don’t realize it. But the program helps them start to help each other and they empathize with each other.
“It’s kind of amazing,” she added. “Take Helen for example. She’s playful now, and everybody knows about Helen at Armbrook.”
The ConnectedLIFE program starts after breakfast each morning. All of the a.m. programming is done in the same place to help people remember where they need to be, an important consideration.
“We had one woman living with dementia who was living independently with her husband. When he died, she moved into assisted living, but kept going back to her old apartment, because she didn’t remember where the new one was,” said Cardillo. “I remembered she and her husband sailed a lot, and I had a nice photo of a sailboat, so I hung it by her new apartment, so that whenever she got off the elevators, she’d follow the sailboat.”
The first activity is really a coffee klatch — a time to look at the daily paper, see what’s going on, what the weather’s going to be, and what happened in history that day. “I want them to realize, ‘yup, it’s August; yup, it’s hot,’ and that it’s normal. That’s what we’re trying to do, normalization,” said O’Donnell.
After coffee hour, there’s usually a cognitive game that gets the women remembering and sharing things like what they fed their kids, or what they did with them in the car on long road trips. “Everything flows from one activity to the next,” said O’Donnell. “The activities are usually about 45 minutes in total, because that’s the attention span we have,” she added. A snack is served midmorning. After the snack, residents take part in a physical game to get them revved up for lunch.
“At this point, their minds are alert,” O’Donnell noted, “and now I want their bodies to be as well. We really focus on whole-brain fitness. It’s the whole package of body, mind and spirit.”
After lunch, there’s another physical game to keep the residents active. When the weather’s good these activities tend to be outside, including games like golf or corn toss.
In the fall, they’ll move inside and into the kitchen for the wonderful aromatherapy of baking. After the physical game, they may move into the den and play bingo or other games.
“We work a lot with reminiscing. We have a lot of books that are … ‘finish the phrase; finish the line; finish the lyrics.’ We do a lot with music. Thanks to YouTube, we can find pretty much anything they want, including Sinatra and Perry Como. They also love cute baby pictures and puppies,” said O’Donnell.
The last half hour before dinner is all about chilling out and cooling down. “These people are tired. They’ve been going since 8 in the morning, so by 4:30, they’re spent, and if they want to take a little snooze before dinner, that’s o.k.,” says O’Donnell.
The final program of the day is after dinner, at 6:15 p.m. While it’s geared to ConnectedLIFE, it’s open to the whole community, which gives residents a chance to see what the program is all about.
Still Growing
Recently, ConnectedLIFE expanded programming to include weekends. “We were hearing from families that when they came to visit loved ones on Saturdays, they didn’t have much to do. We listened to that feedback and added weekend programming,” said Cardillo. “This is way more than a day program.”
Presently, there are 14 people participating in ConnectedLIFE, and Cardillo hopes there will be more.
“We started last September with a small group and have seen about 20 come through the program,” she said. “We don’t know where this is going to take us, maybe a second tract, but for now we know it works.

With ConnectedLIFE, seniors get as many chances as they need to get the bean bag into the hole.
Hodur agreed. “When Helen came here, I was hoping she’d have a friend, someone to get coffee with; well now, she’s got a baker’s dozen friends. It’s so fabulous.”
Families are kept up to speed with quarterly assessments and a bi-annual care plan meeting where they go over goals for each resident. Cardillo also e-mails or texts families weekly to keep them updated and aware of what’s going on.
ConnectedLIFE is another example of how Armbrook Village, one of 14 senior living residences owned, operated and managed by Senior Living Residences (SLR), continues to innovate and create new programs to meet residents’ needs.
Twelve of the SLR communities are in the Boston area, with Armbrook Village the only community in Western Mass. The first ConnectedLIFE program started in SLR’s Canton, Mass. community, and once Cardillo heard about it, she said “we have to do this.”
Cardillo praises SLR for being innovative.
“They’re incredibly progressive, and proactive; every month all of the executive directors meet with the company president,” she explained. “At one meeting, I brought up how we were seeing people walking around, and we weren’t serving their needs, and everyone said ‘that’s a problem for us, too.’ ConnectedLIVING is the end result.”
Canton was a start-up community at the time, she went on, and it was decided to pilot the program there as an opening-up venture.
Cardillo is also proud of another first-of-its-kind educational program that started at Armbrook.
“We have the distinction of being the first Dementia Friendly Community on the east coast,” she noted. “It’s part of a drive to make towns friendlier and safer to those experiencing dementia. We wanted to create an environment where, if an individual with memory loss went into a restaurant or other establishment, staff would know the right steps to handle the situation.”
Every EMT in Westfield has been trained in the program, along with Baystate Noble Hospital, Baystate Noble VNA, Councils on Aging, schools, chambers of commerce, family members, and the community at large.
“My job is really to educate people,” she explained. “We feel it’s really important to prepare people for interactions with someone whose memory may be a little topsy-turvy. We started this campaign here, then all Senior Living Residences decided to do that in their community, and now there’s a whole movement called Dementia Friendly Massachusetts.”
Community Resource
Armbrook Village also provides support groups once a month for people in the community. Presently there are about 15-20 people who attend each month, sharing experiences, advice, and sympathy.
“Our role is to make sure everybody gets a chance to talk, and get their questions answered,” said Cardillo. “It’s meaningful for them, and us. We’ve gotten really close with these people.”
Cardillo said she sees Armbrook Village as an educational resource in the community. “We see a need, and we figure out what to do to meet the need,” she says.
Armbrook offers a variety of options along the continuum of aging, its 122 units encompassing independent living, assisted living, and what’s known as Compass Memory Support Neighborhood, a secure setting where residents receive constant treatment and supervision.
Research-based memory support programs, including Reconnections lifelong learning, and specialized art and music classes, contribute to increased social engagement and greater cognition.
“Four or five women are of Italian descent, so we started to learn Italian,” said O’Donnell. Every day she puts up a vocabulary word for the day and the women practice. “It brings them back to their childhood, and their roots.”
A year ago, Armbrook started a Memory Café for people in the community newly diagnosed with Alzheimer’s disease or other dementias. “We offer a place for folks to go monthly with their caregivers to meet other people like them. It’s not a support group; it’s a chance for them to meet people who have the same stuff going on, and share an activity from yoga and painting to art and ice cream sundae socials,” said Cardillo.
Her next venture, which is still in the research phase, involves a new movement of music therapy called the ‘Giving Voice Chorus.’
“All the current research points to the importance of music in people’s lives,” said Cardillo. “And we’re seeing amazing success stories of people living with dementia coming together and forming a chorus.”
Stay tuned.
“We’ve learned to be flexible,” Cardillo said in conclusion. “We want to give our residents the best quality of life possible, and we keep raising the bar. We work until we get it right.”



 The creator of Principled Heart, a certified financial planner, said his goal was to help answer a common question: where do we keep all our planning documents and information — and how will my loved ones know what to do? His site encourages people to keep only what is necessary, including passwords (or instructions on where to find them) for financial accounts, social media, and other accounts. Other features include instructions for pet care, key contacts, and space to upload up to 60 documents.
The creator of Principled Heart, a certified financial planner, said his goal was to help answer a common question: where do we keep all our planning documents and information — and how will my loved ones know what to do? His site encourages people to keep only what is necessary, including passwords (or instructions on where to find them) for financial accounts, social media, and other accounts. Other features include instructions for pet care, key contacts, and space to upload up to 60 documents.









 When Bec Belofsky married Lee Shuer, she had no idea he had hoarding disorder.
When Bec Belofsky married Lee Shuer, she had no idea he had hoarding disorder.

 SPRINGFIELD — In a time of change for what, until recently, was known as the Assoc. for Community Living, the organization’s passion and innovative spirit will remain constants, its executive director says.
SPRINGFIELD — In a time of change for what, until recently, was known as the Assoc. for Community Living, the organization’s passion and innovative spirit will remain constants, its executive director says.