Problematic Projections
 Even with media and government now intently aware of the opioid crisis, a recent report still projects that 500,000 people may die from these drugs over the next decade. But the groundwork is being laid, through multi-pronged strategies, to stem the tide of overdoses and deaths. It’s a tall order, those in healthcare say, but they’re hopeful.
Even with media and government now intently aware of the opioid crisis, a recent report still projects that 500,000 people may die from these drugs over the next decade. But the groundwork is being laid, through multi-pronged strategies, to stem the tide of overdoses and deaths. It’s a tall order, those in healthcare say, but they’re hopeful.
The projections are, well, to use a term from this realm in healthcare, quite sobering.
Indeed, a report issued by STAT, a national publication focused on healthcare, medicine, and scientific discovery, noted that a team of experts forecasts that the opioid crisis in this country will get worse before it gets better, and that 500,000 people could die from opioids over the next decade.
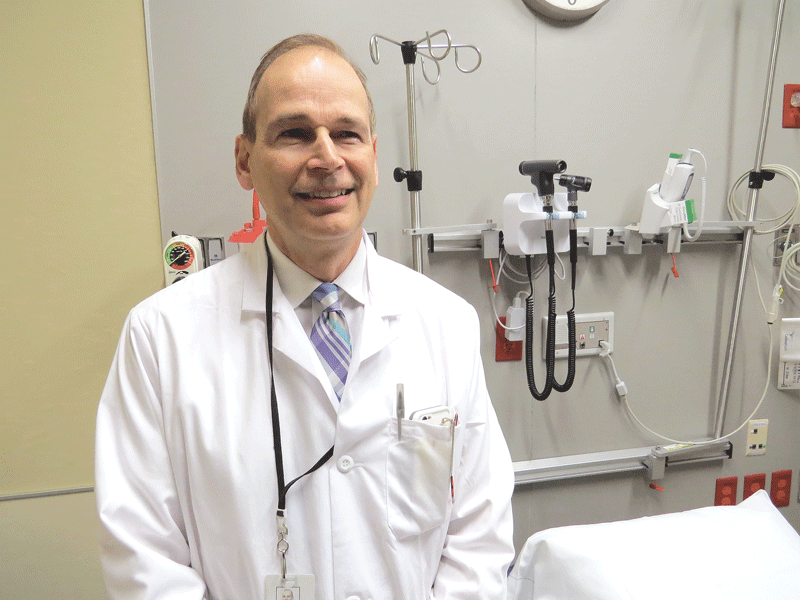
Dr. Peter Friedmann says the culture around opioid use and abuse must change if real progress is to be achieved.
And, unfortunately, that’s not the worst-case scenario.
Those same experts project that the toll could spike to 650,000 over the next decade if potent synthetic opioids like fentanyl and carfentanil continue to spread rapidly and the waits for treatment continue to stretch weeks in hard-hit states.
Most of the forecasts produced by STAT predict the annual death toll will increase by at least 35% between 2015 and 2027. Under the gravest scenarios, it could triple — to more than 93,000 deaths per year.
The report’s alarming projections prompted BusinessWest to reach out to some of those in this region working to stem this tide for input about what will ultimately drive the numbers over the next decade, and what path this crisis will take — toward improvement, or, as those experts quoted in the STAT report suggest, toward even more grave statistics.
There was general agreement that, while there have been some forms of progress with regard to this crisis — in arenas ranging from awareness to treatment — far more profound change will have to come to keep those dire projections from becoming reality. And this change must come in many forms, they said — from reducing the stigma attached to this disease and the proven methods of treating it to curbing the number of opioids prescribed; from allocating far more resources to the fight to compelling more individuals and constituencies to take ownership of the problem.
“The real issue, from my perspective, is that the culture around this disease has been very slow to change,” said Dr. Peter Friedmann, chief research officer and endowed chair for clinical research at Baystate Health, an addiction researcher funded by the National Institute on Drug Abuse, and an addiction-medicine clinician. “There are a lot of people who still view this as a disease that you’re going to cure — you can put someone in the detox for a week or a few weeks, and then you put them in an outpatient program with no medication or anything, and they’ll come, and they’ll be cured.”
Realization that medication-free treatment, or ‘drug-free’ treatment, is not going to stem the tide of overdoses and is, in fact, harming individuals by reducing their tolerance to the drug and leaving them more susceptible to overdose is only one of the factors that go into this needed culture change, said Friedmann, adding that, overall, there is preoccupation (among legislators and others) with creating more ‘beds’ and detoxification, when the focus should be on proven forms of treatment.

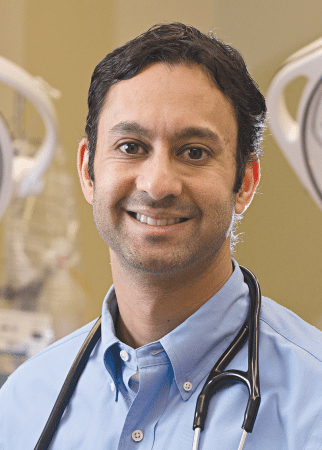
Dr. Robert Roose says individual states and regions have opportunities to fare better than the projections nationally for opioid deaths.
These include methadone, buprenorphine, and naltrexone, he said, adding that there is also a real stigma about these treatments, which ultimately limits access to them.
But amid all the dire projections, there is some room for optimism, said Dr. Robert Roose, vice president of Behavioral Health for Mercy Medical Center and its affiliates. He noted that the STAT report and others like it are national in scope, and that individual states and regions have opportunities to create their own, more impressive patterns for opioid-related deaths.
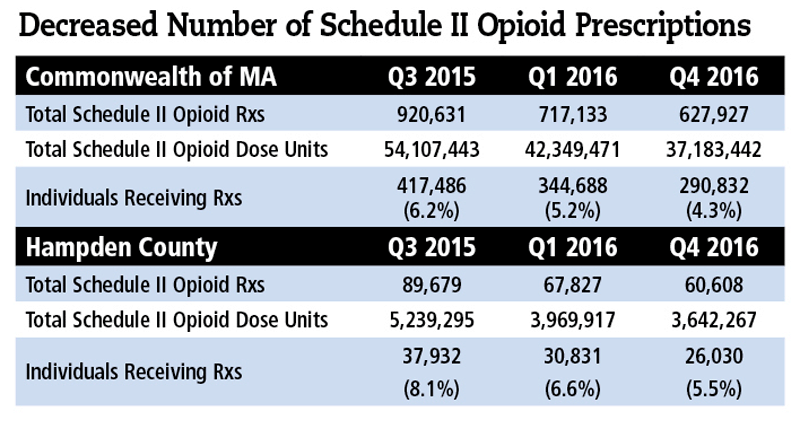
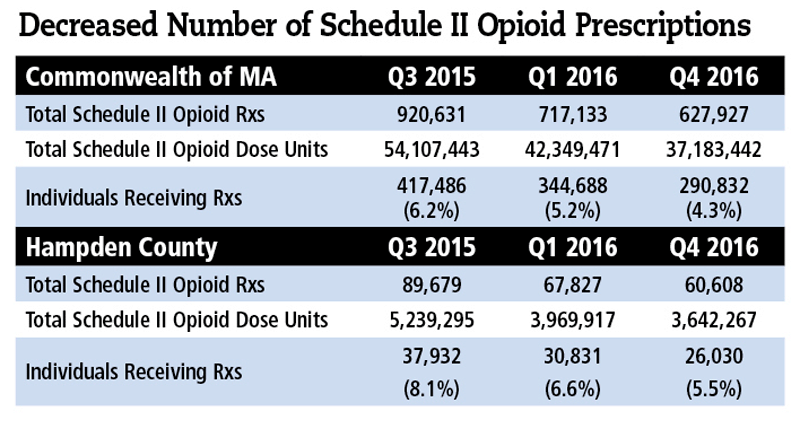
And he believes that both Massachusetts and Hampden County could be ahead of the curve in some areas, including opioid prescriptions. He cited statistics showing improvement in total Schedule II prescriptions and individuals receiving prescriptions, both statewide and in Hampden County, thanks in large part to the Massachusetts Prescription Awareness Tool (MassPAT).
“The hope that I have is that, with some of the strategies that have been implemented in Massachusetts and other states, while we have certainly been hard-hit, we are laying some groundwork to stem the tide and reduce the rate of increase in overdoses in the short term, and in the long term, reduce the rate of overdose deaths,” he said.
Katherine Cook, vice president of Adult Mental Health and Substance Abuse at the Center for Human Development (CHD), agreed, but added that, to achieve progress and a better-case scenario moving forward, cultural changes must take place on many levels, starting with prescription practices and the basic approach to treating illnesses.
“We’re a culture where, for the common cold, for which there is no cure, you can walk into in any drugstore, and there are aisles of remedies,” she said. “That’s how we’re taught to care for ourselves, with a medication.”
There are many components to this opioid fight, said those we spoke with, but overall, the goals are to keep more people from becoming addicted, to treat them properly when they do become addicted, and to provide them with all the tools and resources needed to remain sober.
And these are all very tall orders.
Overall, the experts we spoke with said this country knows what works when it comes to this crisis — everything from stemming the flow of super-deadly synthetic opioids to getting more people access to medications that can reduce cravings — it just needs to do much more of it.
Dose of Reality
As he talked about the opioid crisis and the many projections about what could and probably will be in the decade to come, Friedmann drew many striking comparisons to another crisis that unfolded nearly 40 years ago.
This was the HIV/AIDS epidemic, he told BusinessWest, adding that, during that crisis, as with this one, people were dying, there was a strong stigma attached to the disease (and a reluctance to call it a disease), fear, no shortage of projections about how many people would die in the years to come, and a general reluctance on the part of many parties to take responsibility for what was going on.
“There was a lot of unwillingness on the part of many doctors to deal with those patients,” he said of the HIV/AIDS crisis. “And the notion that it was a disease really only took hold when they identified the retrovirus.”
There is no retrovirus with the opioid crisis, he went on, adding that the stigma attached to this problem persists, and it is only one of the many hurdles to turning the proverbial corner with this epidemic.

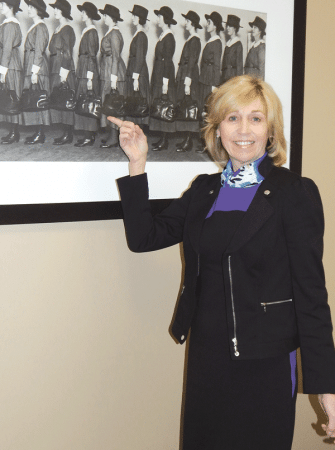
Katherine Cook says one of the keys to achieving progress with the opioid crisis is removing stigmas and the ‘us and them’ philosophy.
But it is a huge hurdle, said Cook.
“We have come a long way, but there’s still judgment and a devaluing of people, and that’s not just in the U.S.,” she noted. “With substance use, it becomes a moral judgment that people impose on others; we need to show that this isn’t an ‘us and them’ situation — we’re all human.”
Like all those we spoke with, Cook said there are a number of factors that will ultimately determine just which trajectory the graphs charting opioid-related deaths will take in the years to come. These include prevention and treatment efforts, obviously, but also issues such as access to healthcare, employment opportunities, and safe, affordable housing.
“It’s not just mental health and substance abuse,” she told BusinessWest. “It’s all of the social indicators of health, and if we don’t look at that, we’re not going to be able to make a difference.
“And it’s not just treatment beds,” she went on, adding, again that more of those certainly are needed. “It’s also recovery homes, what we used to call ‘halfway houses,’ or ‘three-quarter-way houses’ — ongoing support, and the ability for the community to care compassionately about individuals who are struggling with addiction and making sure those resources are there so people can be successful after treatment or recovery. The ability to maintain recovery will ultimately determine if we see a change and maybe the best-case scenario.”
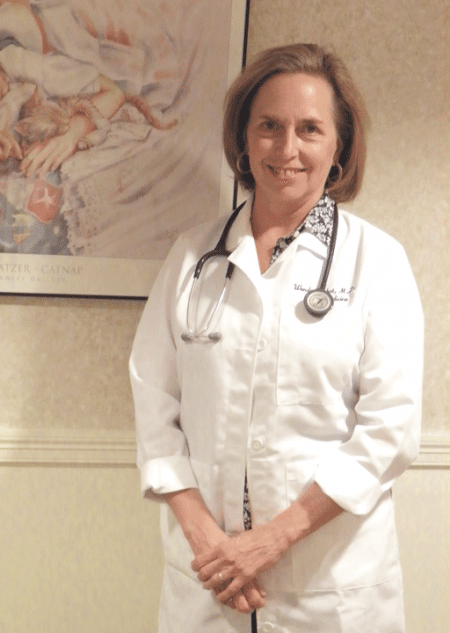
Rose Evans, vice president of Operations in the Substance Use Division for Springfield-based Behavioral Health Network (BHN), agreed. She arrived at the agency only a few months ago after spending the previous four years working for the Patrick and Baker administrations to address individual and family homelessness.

Rose Evans says one key to addressing the opioid crisis is removing the silos around programs involved with prevention, treatment, and recovery.
In that role, she saw some of the enormous toll taken by opioid addiction and the many elements to the state’s opioid crisis.
She said BHN has developed a broad portfolio of substance-use programs over the years, including everything from prevention initiatives in area schools to acute treatment services to outpatient recovery programs. In recent years, it has worked diligently to remove silos and integrate such services. And in many ways, she noted, this is what must happen across the broad spectrum of opioid-use prevention and treatment.
“We’ve been mindful of the impacts that substance use and abuse can have on people and not treating it separately from significant mental-health issues,” she explained. “We’re looking at the social determinants in one’s life and treating it in a comprehensive, multi-disciplinary way.
“What we saw in my previous employment was the intersection of opioid use and homelessness,” she went on. “We understand that there’s a relationship and a correlation between one’s use of substances and the impact it can have on employment, education, housing, family life, relationships, and much more.”
Prescription for Progress
Overall, Roose believes the rate of increase in overdose deaths has at least begun to slow in Massachusetts, a dose of positive news he points to as evidence that individual states and regions can defy the most dire projections. And such deaths, while not the only statistic to chart when it comes to this crisis, is easily the most poignant.
“There’s no question that this is about saving people’s lives,” he explained. “And if we can reduce early death related to this disease, we should be doing everything we can to achieve that.”
Friedmann agreed, but noted that opioid-related deaths are, in every respect, like the tip of an iceberg. They are what can be seen, and they are the focus of the front-page newspaper headlines, but there is so much more lying beneath the surface.
Indeed, there are other important elements and forms of data that must be considered when it comes to the broad efforts to stem the powerful opioid tide, he said, and these include the number of people who struggle with opioid-use disorder or addiction and who don’t have access to treatment, as well as the outcomes from treatment.
The healthcare community currently lacks sufficient data in such areas, Friedmann said, adding that better numbers could help in the formation of specific strategies for dealing with the crisis moving forward.
One statistic that he can track is the number of beds, which has increased significantly over the past several years, both statewide and in this region. And the beds have come in several varieties, he noted, including those related to inpatient psychiatric care, detox care, and in-patient stabilization and longer-term transitional support.
“That is definitely providing more access to people who did not have access before,” he said of the increase in beds. “It doesn’t mean that we’ve caught up to the demand by any means, or that there aren’t other areas of the system that need to be increased, but there has definitely been a significant investment on the part of the state to provide more access to care.”
But access is still an issue — waiting lists prevail in this state, and they are considerably longer in harder-hit states such as West Virginia and New Hampshire — as is the matter of providing the right kind of care.
Friedmann said he is currently writing a paper on the broad subject of ‘beds’ in relation to the opioid crisis. The thesis, he told BusinessWest, is that the detoxification system for opioids should be re-engineered, as he put it, with creation of a “system of induction centers,” rather than a system of detoxification centers.
We need to remove from our bodies what we can by way of detox. But then, to send someone back out into the same pasture to eat the same grass is not going to do that individual any good. We need to be able to look at the person holistically to see what they need, and if medication-assisted treatment is what’s going to help them develop the skills to manage in the world and in the environment where they’ve been using, then that’s going to be a lifeline for them.”
“What we should be doing is getting people to get on medication and stay on medication,” he explained, adding, again, that detoxification generally leaves individuals more susceptible to overdose if they relapse, and a huge percentage of such patients eventually do.
Cook agreed. “We need to remove from our bodies what we can by way of detox,” she said. “But then, to send someone back out into the same pasture to eat the same grass is not going to do that individual any good. We need to be able to look at the person holistically to see what they need, and if medication-assisted treatment is what’s going to help them develop the skills to manage in the world and in the environment where they’ve been using, then that’s going to be a lifeline for them.
There are, of course, many other ingredients in a broad formula for progress and creating greener pastures, if you will, said those we spoke with.
They include prevention, safe prescribing, more effective recognition of individuals’ opioid problems, taking immediate steps to curb the availability of fentanyl and carfentanil, and also the development of a qualified workforce to care for those with opioid issues.
The sheer number of hurdles and the complexity of each one combine to create an enormous challenge and, indirectly, those dire predictions moving forward.
“There are so many moving parts when it comes to this disease, and that’s what I find so fascinating about it,” said Friedmann. “And we have to address all of them simultaneously.”
Moving the Needle
Summing up matters succinctly and poignantly, Cook said that, to stem the tide of opioid use and abuse, “we have to keep working hard every day.”
And keep working on a number of fronts all at once, she went on, speaking for all those we interviewed, because there are many layers to this crisis. Only by slicing through all those layers, experts say, can this region and the nation keep the worst-case scenarios from becoming reality.
Friedmann might have said it best when he told BusinessWest, “this is a crisis people talk about, and increasingly we’re seeing some action, but it can’t really come fast enough.”
George O’Brien can be reached at [email protected]









 As the Baby Boom generation continues to hurtle into their retirement years, about 15% of all Americans today are over age 65, a percentage expected to soar to almost 22% by 2040. That demographic tide presents both challenges and opportunities for senior-living facilities, which more than ever are emphasizing a continuum of care and a resident-centric experience.
As the Baby Boom generation continues to hurtle into their retirement years, about 15% of all Americans today are over age 65, a percentage expected to soar to almost 22% by 2040. That demographic tide presents both challenges and opportunities for senior-living facilities, which more than ever are emphasizing a continuum of care and a resident-centric experience.



















 Keroack is board-certified in internal medicine and bariatric (weight-management) medicine, and originally built his practice around weight loss, moving gradually into a broader wellness focus, where patients lose weight as just one benefit of a total lifestyle shift. But in addition to his formal training, he has certifications from the Institute of Functional Medicine and the Cenegenics Education and Research Foundation for Age Management Medicine.
Keroack is board-certified in internal medicine and bariatric (weight-management) medicine, and originally built his practice around weight loss, moving gradually into a broader wellness focus, where patients lose weight as just one benefit of a total lifestyle shift. But in addition to his formal training, he has certifications from the Institute of Functional Medicine and the Cenegenics Education and Research Foundation for Age Management Medicine.